By Helen Kimball-Brooke MARH, guest author
A press conference on the Gardasil vaccine was held in Paris on Wednesday the 2nd April 2014 at the local offices of the European Parliament, a short walk from the French National Assembly. It was organised by MEP Michèle Rivasi (Vice-Chair of the Greens/European Free Alliance group) who has held meetings in the past on pharmacovigilance in Brussels and other press conferences on the aluminium salts used as adjuvants in vaccines, in Paris. Three members of EFVV (the European Forum for Vaccine Vigilance) attended the conference: myself, Françoise Joët from the French group ALIS and Dr. Françoise Berthoud, retired homeopathic paediatrician from Switzerland.

Aside from Michèle Rivasi, the speakers included the parents of two HPV-vaccine victims: 18-year-old Marie-Océane Bourguignon who after receiving two doses of Gardasil at age 15 now suffers from multiple sclerosis (MS) and Orianne Lochu, age 21, a former first-year medical student now struggling with severe macrophagic myofasciitis, an illness thought to be linked with the aluminium adjuvants in vaccines. Both HPV vaccines, Gardasil and Cervarix, contain aluminium salts. Within months of her jabs, Océane, the only French HPV vaccine victim for whom the link to the vaccine has been officially recognised by a Medicine Injury court, temporarily lost both her sight and the use of her legs after being hospitalised for what appeared to be either acute disseminated encephalomyelitis (ADEM) or multiple sclerosis.
Océane’s case was originally heard by the Bordeaux Commission de Conciliation et d’Indemnisation or Medical Accident Arbitration and Compensation Committee, set up by the Ministry of Justice with members appointed by the local Public Health Authority. As of the judgement in September 2013 she was awarded compensation amounting to 50% of her claim but given that Sanofi-Pasteur were clearly incriminated in the case and thinking of all the other victims, her parents chose to forfeit the compensation by filing charges in the criminal courts. The criminal court case is still pending.
The parents of both girls expressed anger and frustration over the way they had been treated: refusal by the medical profession to acknowledge that their daughters’ illnesses had been triggered by the vaccine, lack of support and treatment for the girls’ ailments, even suspicion and ostracism for having dared to blame the vaccine. The experience has been all the more difficult for Orianne’s parents who are medical professionals themselves: her father is an anaesthesiologist and her mother a nurse.
Océane’s lawyer, Maître Jean-Christophe Coubris, also defending over 100 other French HPV-vaccine victims, was another speaker, as was Serge Rader, a pharmacist who has done research on the widely varying prices of vaccines across Europe, and Elena Pasca, a philosopher, member of the board of Sciences Citoyennes and author of a blog called Pharmacritique, who discussed the conflicts of interest inherent in the development and marketing of these vaccines.
Others present included French medical consultants Profs. Authier and Gherardi, doing research on the aluminium salt adjuvants in vaccines at the Henri-Mondor Hospital in Créteil, a Parisian suburb, and consultant Dr. Laurent Belec, head of the virology laboratory at the Georges Pompidou European Hospital in Paris. The sudden withdrawal in 2013 of the funding for the important work of Authier and Gherardi was the topic of another press conference organised by Michèle Rivasi last year. Their funding was only re-instated after two members of the NGO victim support group E3M went on a hunger strike.

The speakers of honour however were Drs. Christopher Shaw, neurologist, and Lucija Tomljenovic, PhD, from the University of British Columbia, Canada, known for their research on Gardasil and the dangers of its adjuvants. Currently doing research with Professor Yehuda Shoenfeld in Tel Aviv, Israel, on vaccine adjuvant-induced autoimmune diseases, they spoke of the effects on the body of the aluminium in vaccines. It has been shown that aluminium migrates through the body to the brain, where it accumulates, potentially causing many adverse effects: convulsions, fainting spells, Guillain-Barré syndrome, transverse myelitis, facial paralysis, chronic fatigue syndrome, autoimmune diseases, pulmonary embolisms, macrophagic myofasciitis, pancreatitis and even death.

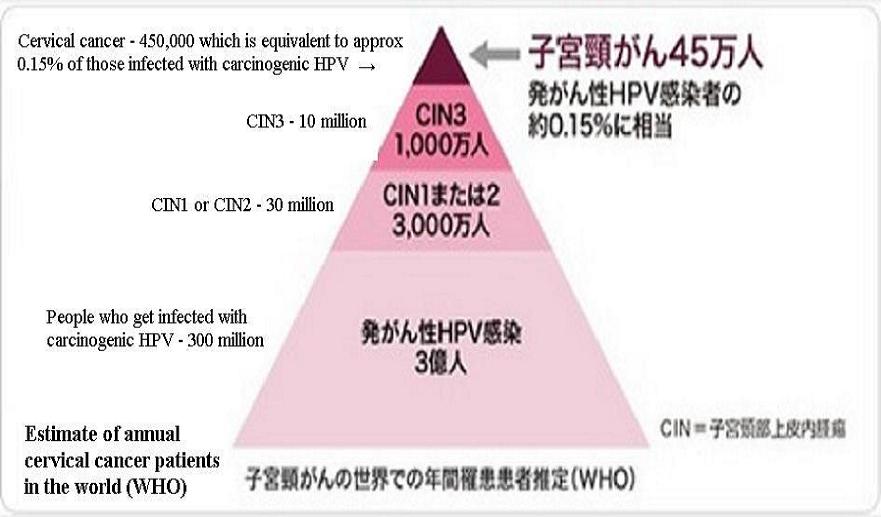
Dr. Tomljenovic demonstrated how these vaccines were rushed prematurely to market. In the USA, the FDA approved the vaccine very fast, reflecting, in her opinion, the flaws and incompetence which are now sadly a characteristic of the organisation. Development of cervical cancer from HPV infection is in fact very slow and 90% of HPV infections resolve of their own accord within three years. The duration of follow-up in the clinical trials was only 4.5 years for Gardasil and 8.4 years for Cervarix but given the slow growth of these cancers, at least 15 if not 20 years would really be needed to establish accurate efficacy. The manufacturers have nonetheless claimed 70% efficacy based on these short-term trials, and Sanofi-Pasteur, who market Gardasil for its manufacturer Merck, have even claimed ‘up to 100%’ efficacy while true vaccine efficacy could be as low as 16.9%.
STIKO, the German Standing Vaccine Committee’s flawed assumption that the vaccine would confer lifelong protection of 92.5% led to the decision to reimburse the HPV vaccine in Germany and incited many German doctors to recommend it. Since its introduction 7 years ago, nearly 2 million young French women between the ages of 13 and 26 have received at least one dose of Gardasil, reimbursed at 65% by the Social Security, even though its effectiveness has not yet been proven and is highly controversial. There are in fact over 100 strains of HPV but Gardasil contains only antigens from strains 6, 11, 16 and 18, considered the most oncogenic. Strains 16 and 18 are responsible for 70% of cervical cancers which is why these are the only two in Cervarix but infections with these two strains also seem to be less common in Europe. In fact, cervical cancer represents only 1.7% of all cancers in France so it is not actually a public health problem there anymore.
On the 4th of February 2014 however, President François Hollande announced that as part of his ‘Cancer Plan’, he wanted HPV vaccine uptake amongst young French women to double over the next five years. This came as an enormous shock to the parents of the 10 girls with very severe neurological complaints, who by November 2013 had already initiated legal proceedings against both Sanofi Pasteur and ANSM, the French national medicines safety authority.
To quote Dr. Tomljenovic:
‘Just as pizza-bearing cheerleader drug reps are a poor substitute for medical education, pharmaceutical lobbying is a poor substitute for well-reasoned public health policy-making….Is it ethical to put young women at risk of death or a disabling autoimmune neurodegenerative disease at a pre-adolescent age for a vaccine that has not yet prevented a single case of cervical cancer, a disease that may develop 20-30 years after exposure to HPV, when the same can be prevented with regular Pap screening which carries no risk?’
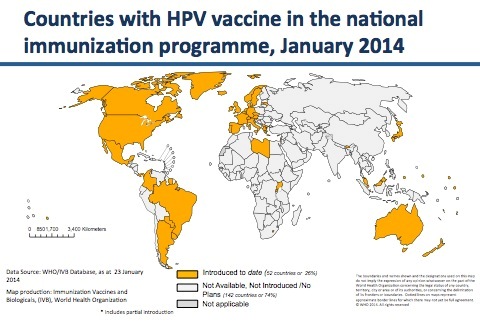
The number of HPV vaccine victims continues to grow in France and worldwide, with some countries taking a more cautious stance: Austria refused from the start to include the HPV vaccine in its vaccination schedule and during 2013, under pressure from victims, the Japanese Ministry of Health, Labour and Welfare withdrew its recommendation for the HPV vaccine. Shortly after the press conference in Paris, it was announced in Japan that instead of reinstating the HPV vaccine recommendation, the authorities would hold off for at least another year.
On the 30th March, only three days before the press conference, it was reported in French newspaper Journal du Dimanche that 420 French doctors plus nearly another 300 pharmacists, midwives and other medical professionals had signed a petition demanding a parliamentary mission to reassess Gardasil, claiming that its effectiveness is limited (only 20% according to clinical trials) and its cost exorbitant. They also fear that the vaccine may mislead women into thinking that a Pap smear, whose effectiveness has been proven, is not necessary. As of late May 2014, there were nearly 1200 signatures on the petition.
Of course a counter-petition was also launched by seven scholarly medical groups affirming the benefits of the vaccine but speaking of cost: what in fact is the actual cost of this HPV vaccine campaign in France? Mr. Rader informed us that a single dose of Gardasil costs €123.44, compared with prices ranging from €6.50 to €57 for other French vaccines, the prices of which have increased as new vaccines were introduced over the years. The three jabs required would therefore come to a whopping total cost of €370.32 per individual. The duration of protection conferred by the initial vaccination is still not known so the overall cost would increase if boosters were required. A ‘catch-up’ period could generate a cost to the French Social Security of a shocking €926 million and in subsequent years, the annual cost would be €148 million. What incites more questions however is that a single dose of Gardasil costs only €60.50 in Italy and the Rotavirus vaccine recently recommended for all new-borns by the French High Council for Public Health, costs €54.60 per dose, including tax, compared with only $1 per dose in India. Why do vaccines cost so much in France?
Pap smears, costing €15.40 each in France, remain the best and most effective way to fight cervical cancer. The speakers therefore questioned why the French government was so intent on pushing Gardasil whose effectiveness is debateable and will not be known for 15 or more years, let alone its excessive cost. An indecent communication campaign with lobbying and aggressive advertising was apparently engaged a number of years ago to promote this vaccine. The adverts played on the fears and guilt especially of mothers and in 2010, one of them was even banned for ‘lack of objectivity’ by the French Medicines Agency.
Mme. Rivasi therefore concluded the press conference with a forceful:
‘Enough is enough! It is time to demand a moratorium on this vaccine! EU member states must stop recommending this vaccine until more studies are conducted on Gardasil, its effectiveness and its dangers.’

Less than two months later, her efforts seemed finally to be having some effect: on the 22nd May, under pressure from victim support groups, primarily E3M, an NGO supporting patients with macrophagic myofasciitis, two colloquia with round-table debates open to the public and in the presence of the press, television and even French Health Minister Marisol Touraine, were organised at the French National Assembly: one in the morning by E3M and facilitated by journalist Viginie Belle, the other in the afternoon by Office parlementaire des choix scientifiques et technologiques (Opecst, similar to our House of Commons Science and Technology Committee).
A fair number of the speakers from the April press conference (Gherardi, Authier, Shoenfeld, Orianne Lochu’s mother, Tomljenovic, Belec, Rivasi) took part, alongside representatives from Sanofi-Pasteur, GSK, the French government and other scientists promoting vaccines. Pro-caution and pro-choice scientists also included our own Prof. Christopher Exley from Keele University, Dr. Lluis Lujan, veterinary pathologist from the University of Zaragoza in Spain and Prof. Michel Georget, French biologist and author of books on the adverse effects of vaccines.
Topics of the four round-table debates: 1) Aluminium: Adjuvant under Scrutiny. 2) HPV Vaccine: Time to Exercise Caution, in the morning. Then in the afternoon: 1) The Safety and Efficacy of Aluminium Vaccine Adjuvants. 2.a) Is a Moratorium Appropriate? 2.b) Are there Alternative Vaccine Adjuvants?
For those who speak French, these debates can be viewed here: http://videos.assemblee-nationale.fr/video.5464. Compared with our House of Commons Science and Technology Committee’s Evidence Check into Homeopathy in 2009, this series of debates seemed far more balanced! The focus in France seems at present to be only on aluminium, which may not be the only issue but time will tell as to where it takes the whole French and European vaccine debate.
Knowing that the French Health Minister attended these colloquia and is therefore now fully aware of the latest research on the damage caused by aluminium adjuvants and the Gardasil vaccine, it came as a shock when instead of calling for a moratorium she later reaffirmed the French government’s intent to vaccinate all young French women with this vaccine. Yet another debate was then organised on the 23rd of June by a group of galvanised GPs from La Réunion island, one of France’s overseas departments. The thrust of this series of medical and statistical presentations, again hosted by Michèle Rivasi, was that HPV vaccination is not needed to prevent cervical cancer, is excessively costly and the whole vaccine development and marketing process is fraught with conflicts of interest. Gardasil is clearly a hot topic in France with articles, blogs, petitions and debates appearing frequently. The doctors, researchers, support groups and victims behind these are not about to give up the fight for both a moratorium on Gardasil and aluminium-free vaccines in general.
Remember that in the USA and the UK, HPV and other vaccine victims are fortunate to have SaneVax (http://www.sanevax.org) who in addition to providing the necessary information for making an informed choice, can locate appropriate medical/legal assistance in the event of an adverse event post-vaccination.
Since the April press conference, the EFVV has prepared a Manifesto in English, French, Spanish, Italian, German, Dutch and Slovenian (other languages possibly to follow), demanding the abolition of mandatory vaccination in the EU (see http://www.efvv.eu). The plan is to launch a petition based on this Manifesto and a delegation of EFVV members will be meeting with Michèle Rivasi in September to discuss the best way to utilise these documents and submit their demands to the European Parliament. Watch this space, both in France and Europe-wide.
(Note: This article was originally written for Homeopathy in Practice, the journal of the Alliance of Registered Homeopaths in the UK but, with kind permission of HIP, is appearing here first.)
Article compliments of SaneVax.org