By Freda Birrell
We would like to thank Luciana Berger, MP Shadow Minister for Public Health, her Parliamentary Assistant Kat Thompson, The Countess of Mar from the House of Lords, Pat McFadden, MP, Joe Benton, MP, Mary Creagh, MP and Tom Fieldhouse, researcher in the office of Oliver Letwin, MP for taking the time to meet the parents and girls who had an adverse reaction to the HPV vaccines.
From the presentations given we would like to highlight a few very disturbing points which we hope Ms Berger will take on board and ask relevant questions. The points made are not unique to this group of families from the United Kingdom. They are the same for many families around the world.
- Serious loss of education and the opportunity to interact with their peers socially;
- Young girls’ mental health being questioned without justification; psychiatric care being promoted time and time again;
- Threatening behaviour towards families by health care officials;
- Families being accused of fabricating their daughters’ illnesses;
- Inadequate duty of care from health care officials;
- Lack of knowledge by medical doctors and consultants on how to recognize and treat the vaccine injured;
- Medical doctors who believe illnesses were caused by the HPV vaccines but are too afraid to speak out.
This sadly is how it is in the UK at the present time. A very important point was made below, ‘these are real people in real situations and it does not matter whether it is a Conservative or Labour government, as politicians you are elected to speak on our behalf and work on our behalf at all times.’

All these families ask for is to be respected, to be listened to and, most importantly, to be believed.
The undernoted presentations were given by girls who were injured by an HPV vaccine and parents speaking on behalf of their daughters.
Julie Jones, mother of Stacey Jones, Bilston, Midlands:
My daughter Stacey had her first Cervarix vaccine on 15th November 2008, aged 17, and we noticed that her mood changed following this vaccination. After the second jab in January her aggressive behaviour was more noticeable and then after her third vaccination in May 2009 she became very disorientated which increased in intensity, couldn’t sleep and that was followed by partial seizures which then developed into full blown seizures.
There were many serious faults here with the NHS, not treating our daughter correctly, sending her to a psychiatric hospital which could not help her but thankfully they recognised her illness was a medical illness and she was sent home.
New Cross Hospital at that time let us down badly and that was when I made contact with my MP, Pat McFadden. Pat gave my family a lot of support for which we are very grateful. Over a period of time Stacey was allocated a place at the Brain Injury Rehabilitation Trust – Stacey spent 12 weeks there relearning simple tasks and she was also assigned a neurologist from the Queen Elizabeth Hospital in Birmingham.
Stacey was officially diagnosed with Anti-NMDA receptor encephalitis – an autoimmune form of encephalitis – NOT VIRAL ENCEPHALITIS. According to NHS Choices, in ‘rare’ cases this condition has followed vaccination. It is strange then that at the same time a young girl called Paige Brennan also from the Midlands was vaccinated with Cervarix and was also diagnosed with the same autoimmune condition as Stacey – not so rare after all.
Now after five years of great improvement in Stacey’s health and being able to go to University, we are devastated that she has had a re-occurrence of this autoimmune form of encephalitis – Stacey was admitted to hospital where she received the best of treatment which was so much better than the last time – I can report she has just been allowed to go home with further rehabilitation to take place. What does the future hold for our daughter – according to the MHRA there are no serious adverse reactions to the Cervarix vaccine – well that is not the case.
Ashleigh Cave, Liverpool:
My name is Ashleigh Cave and I received the HPV Cervarix injection in October 2008 when I was twelve years old. Within an hour of having the injection I had extremely bad headaches. I was going for a routine doctor’s appointment and the doctor said I was suffering from possible side effects of the vaccine and that I should start to feel better in the next forty eight hours. Only I never and over the course of the next week I suffered from severe flu like symptoms and I had no energy to stay awake.
My legs became so weak that I was admitted to hospital as I couldn’t walk or move my legs. I suffered with excruciating pain and was put on a concoction of eight different painkillers. I had tests, scans and x-rays yet they all came back inconclusive. At this point, the doctors didn’t know what was wrong and came to the conclusion that my health issues were psychosomatic. I had to have a full psychiatric assessment which came back in my favour that my health problems were not in my head. So their next move then was to try and blame my mum. They got social services involved and we were threatened that I would be taken into care if my mum did not stop speaking to the press. All in all I was in Alder Hey Children’s hospital for twelve months where I had intensive Physio and Hydrotherapy sessions daily.
I can now walk, however I am limited as I have never fully regained the strength back in my legs. I had health problems before I had the injection, such as Noonan syndrome, pulmonary stenosis, bronchomalacia, bladder problems and chronic asthma. Since I had the injection, everything I previously suffered with was intensified. I have had three surgical procedures to try and help my bladder so I do not have to rely on self-catheterising and administering treatment weekly and I am constantly picking up every cold that is going meaning I am quite frequently in hospital as it affects my chest.
Every girl who has had a reaction has had different health backgrounds, some having previous medical problems and some having a clean bill of health. Some girls have been affected in different ways ranging from paralysis, to having seizures daily but the one thing we all have in common is the fact we have all received this injection. The past five and a half years have been horrendous for me and my mum but what makes it worse is the fact that girls are still having this injection and are still being damaged.
How many more girls have to go through this before someone will take notice and listen? How many more families have to be blamed before being offered support and finally how many more lives have to be turned upside down before we get the recognition and medical help we need for what we are going through?
Emily Ryalls, Ossett, W. Yorkshire:
Hello, my name is Emily. I’m 16 years old and have just completed my GCSE year in high school.
I’d like to thank you for this opportunity to share my experience of the HPV vaccination as well as being able to speak on behalf of other girls. I’m incredibly nervous, as you can probably tell, but so grateful for you taking the time to listen to me today.
I had the HPV vaccination 3½ years ago. I became ill after the first jab, the 2nd jab worsened my condition and after the third jab the visits to A&E started. At first I had complete faith in doctors. Then I was labelled with ME/CFS and I realised this meant that doctors didn’t know what to do with me.
I was so ill, I was missing lots of school, missing my friends and the only treatment given was to see a psychologist. My paediatrician wanted me under the care of a psychiatrist. Every doctor I saw refused to consider vaccine damage and none of them reported it.
After 2 years and a lot of research, we found a specialist who confirmed I had POTS – Postural Orthostatic Tachycardia Syndrome, which is a dysfunction of the autonomic nervous system. Everything that the body should do automatically doesn’t work properly for me, especially when I’m sitting or standing up. It affects every part of my body – eyesight, heart rate, breathing, blood pressure, digestion and especially cognitive problems, which I hate the most because I often feel humiliated in school and it’s affected my education so much.
I’m finally under a neurologist who is trying to help me and who has confirmed my POTS is a result of vaccination.
The only thing that has got me through the last 3 years has been the support of my mum and family and having such a great group of friends. I can’t begin to imagine how hard it is for the girls who don’t have this support.
Although as a group, we all have different stories; we all share the HPV vaccination as the trigger. The question is how many more girls have to go through this before something is done?
Thank you.
Brianna Price, Newport Pagnell:
I’m Brianna, and I’m 15 years old. I had my first and only dose of Cervarix in September 2011, when I was 12 years old. I then experienced my first symptoms 3 weeks after in October, when I’d just turned 13. I went to my GP and had a wide range of tests done but they all came back negative. 6 months later I was diagnosed with CFS/ME by a Great Ormond Street consultant.
Before the jab I’d represented my school in athletics and won them medals, been dancing since I was 2 – I’ve now had to stop this, performed at the Royal Albert Hall and even done some TV work in a BBC drama series.
In the beginning of being ill I was bullied at school. I had people laughing at me, saying I was faking, and even hurtful comments like ‘why aren’t you dead yet?’ I’ve lost all of my friends but one friend because I wasn’t in school and I couldn’t go out with them so now I’m just not invited anymore. It has taken 2 ½ years to get me from 0% attendance to 30% in school, with me doing 12 hours a week maximum.
I have 6 monthly paediatrics and Great Ormond Street check-ups and monthly psychology and physiotherapy sessions. (I got discharged from CAMHS because it wasn’t helping). I have to take tablets to sleep. If I don’t take the tablets I don’t sleep at all that night. I also have chronic back pain which I’m on medication for and when it’s at its worst I can’t breathe properly because of it.
Since then I have also been diagnosed with Raynaud’s, hypermobility and postural hypertension.
My mum thought it was the best idea to allow me to get the vaccine, but if we knew then what we know now about it, I would never have had it.
When we first saw the Great Ormond Street consultant we asked him did he think the vaccine had caused my illness. He replied, “All I can say is I’m treating a lot more girls following the vaccine.”
Presentation with reference to the autoimmune condition Alopecia:
(For the sake of her daughter, mum is not sharing her name – but she presented in full to the Shadow Minister)
My daughter is 13- the youngest of our 3 children. She has 2 older brothers aged 18 and 21. We are a very close knit, fun loving, happy family and all 3 children are extremely close.
Sport and particularly swimming is in the family, the lads have won medals at national level and my daughter has club records. She also has a gold medal for gymnastics and trampolining. She used to play water polo for fun.
She had her 3 Gardasil HPV immunisations, for genital warts, in October 2012 then January and April 2013. On each occasion she had a significant reaction and with hindsight we wouldn’t have let her have number 2 and 3 but we can’t turn back the clock now! She was lethargic, had muscle fatigue, lost her appetite, stopped her beloved sport and had time off school (unheard of) and her periods stopped. In April 2013 following her 3rd jab her hair started falling out in clumps, she lost her eyebrows, lashes and by the summer of 2013 she was totally bald.
I want to share with you the medical professions reaction as I believe this helps mask the bigger HPV picture…
One Dr said and I quote, “These things happen and Jemma needs to move on…”
Another, “This is quite common around the 12/13 year age group”…not surprising in my mind since this is when the immunisation is given.
When confronted with the possible link, the doctor was extremely dismissive and didn’t offer the opportunity of yellow carding the vaccination (which I believed was meant to be a procedure carried out post thalidomide). I did this under my own steam and told him retrospectively what I had done. I was not popular for taking this course of action.
This may be why the recorded numbers of side effects are quite low…..you have to be proactive….
Friends who are GPs have said off the record that Gardasil was and is the cause of her ill health; but for fear of the backlash are not prepared to put their heads above the parapet.
In summary, she no longer does any sport, her school attendance is poor due to total lack of energy, and she sleeps 14+ hours a day and her periods have still not started. Her lack of hair has turned her from a fun loving outgoing and positive person into a self-conscious and reclusive child.
We have explored every avenue for antidotes and suggested courses of action but this has been done with no backing from the very people who should be there to support us.
Clare Ramagge, Reigate, Surrey:
In 2009, Dr Jawad paediatric consultant, demanded why I had allowed my daughter to have the third Cervarix vaccination? We were advised that he had previously highlighted the link between the vaccination and side effects of arthralgia and he verified this concern to Crispin Blunt MP for Reigate. Mr Blunt successfully secured a debate in Parliament to highlight the fact that formally fit healthy young girls were experiencing a number of severe adverse reactions. He highlighted the fact that there was a lack of a robust compensation scheme or mandatory warning system to report such adverse reactions and he questioned the suitability of school as an environment in which to vaccinate children.
In Rebecca’s case, when standard treatment did not cure her, concerned paediatricians brought in multi-disciplinary teams. As described by Dr Leonard Jason, social psychologist,”As a group otherwise caring professionals can commit acts of cruelty that they would not be capable of as individuals.”
We were threatened with legal action if we did not agree to her being sent to a lock up psychiatric unit for eating disorders even though she did not have an eating disorder. They tried to put different labels on her but never diagnosed a psychiatric problem and tried to Section her. After 16 months, a new social worker to Rebecca’s case, with the advice of Dr Nigel Speight, Lady Mar and a solicitor secured Rebecca’s discharge from the unit. Rebecca is still very poorly but being cared for at home by her family, GP, Nurses, nutritionist and a consultant lead. This consultant, an immunologist who also specialises in ME/CFS, explained to the GP that it is likely that it was the Aluminium in the vaccine that triggered Rebecca’s very severe ME.
On all of Rebecca’s notes there is reference to her deterioration starting straight after the first vaccination. 2 consultants have made reference to the vaccine, one to query why she had been allowed to follow through with it and the other to point out the link with Aluminium being the trigger. Rebecca will never get back the 6 years she has lost as a consequence of having this vaccine and we as a family will never recover from the treatment we have received from some of the so called professionals involved in this case. Rebecca remains positive and hopeful of a recovery but like all the other girls affected, she deserves to have recognition as to the vaccine being the cause, she deserves better treatment and better support.
Points raised by Steve Hinks, Carol Green and John Ramagge:
Steve Hinks:
Before the meeting with Luciana Berger, MP, Shadow Minister for Health we held a pre-meeting with other political representatives. During the discussions we were advised that our daughters are what are known widely as ‘vaccine collateral damage’ i.e. unintended casualties. We were grateful for this open and honest comment which is certainly not typical of the Department of Health and National Health Service because most of the families have been told many times, and in writing, that this vaccine is safe and the many side-effects reported are not attributable to the vaccine. In fact many families are blamed for causing the unexpected and inexplicable illnesses and investigated for Fabricated or Induced Illness (FII, previously known as Munchausen’s Syndrome by Proxy). Not content with turning the blame on parents many NHS health professionals have told blatant lies to FII investigators which can be proven by their own material evidence obtained under the Freedom of Information Act (FOIA).
We were also advised to sum up our expectations in a maximum of just two points for maximum effect, rather than a long list.
- Point 1: The DoH and NHS must share the truth and facts related to the HPV vaccine and investigate the unexplained illnesses rather than blame the parents. These investigations should be coordinated at national level. We have many examples of statements in writing from Health Directors and Consultants that this vaccine is safe and not the cause of the adverse reactions, yet the number of Yellow Card reports to the Medicines and Healthcare Products Regulatory Agency (MHRA) is 10 – 100 times more than for the other common vaccines. Statistics obtained from the MHRA under the FOIA were presented to Ms Berger. In 5 years the number of reported reactions to HPV vaccine is 16,726 of which 2,661 are considered serious, including four deaths. Parents also highlighted that they had been discouraged from raising Yellow Cards.
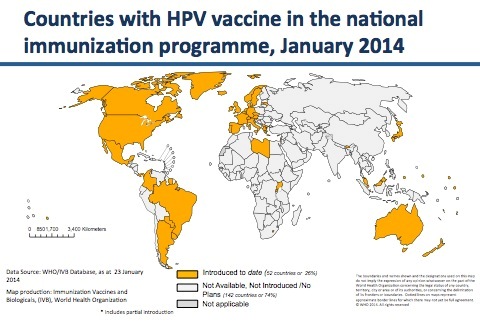
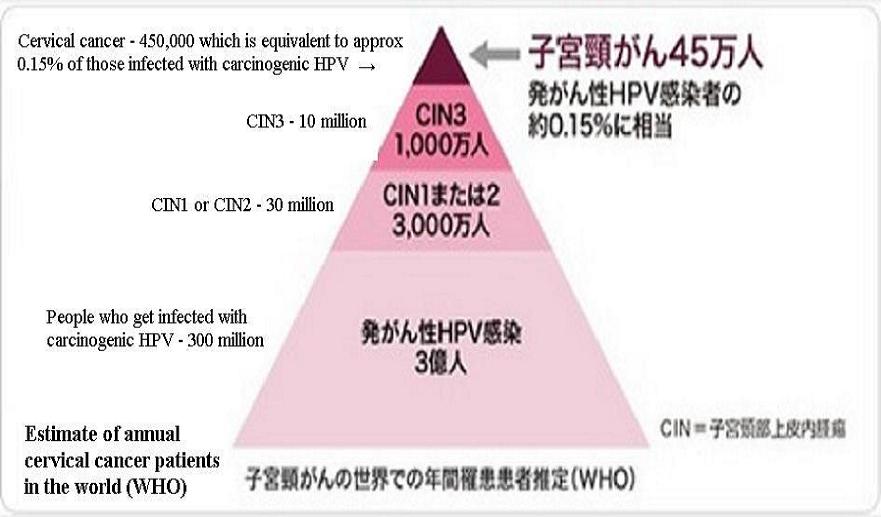
- Point 2: Collateral damage arises in different quantities – it can be small or large and those agencies involved in collateral damage usually at least take preventive action to reduce and minimise it. Given the data reported to the MHRA it is evident that the quantity of reactions reported by Yellow Card are significantly more than for any other vaccine and therefore the use of this vaccine must be stopped until it can be proven to be ‘reasonably’ safe. It must be remembered that this vaccine is expected to reduce incidence of cervical cancer but so far there is no evidence that it will and, since it is accepted that it is not effective against over 15 types of HPV which can cause cervical cancer, the Smear Test will always have to be in place, irrespective of immunisation. This test is safe, extremely efficient and cost effective.
Carol Green, mother of injured young woman Katie:
For the Minister to consider that a consultation by the NHS and government should be a top priority in order to review guidelines when a child presents at hospital or GP surgery with a possible adverse reaction to a vaccination. If this was to become a reality, rather than being dismissive, there would be a set of clear procedures for physicians and doctors to follow to establish whether the vaccine was the likely cause or not. Then appropriate treatment and support (both emotional and financial) can be given to the children and their families so that they would not have to endure what so many families have gone through since the HPV vaccination programme was introduced in the UK in 2008.
As the HPV programme had been promoted and underwritten by the government, they are responsible for ensuring these children receive adequate recognition and compensation if the vaccine is considered to be the cause of their injuries.
John Ramagge:
John pointed out to the Minister that his MP, Crispin Blunt had introduced his daughter’s case to parliament in May 2009 and at that time Labour was in government. This had followed the Minister’s claim that as she was not in government at the present time, there was little that she could do. In 2009, the very questions and points raised by Crispin were belittled by Dawn Primarolo but John wished to make the Minister realise that although she is in shadow government at the moment, as a politician she and her colleagues need to take this matter seriously. These are real people in real situations and it does not matter whether it is a Conservative or Labour government, as politicians you are elected to speak on our behalf and work on our behalf at all times.
All that families ask is to be respected, to be listened to and, most importantly, to be believed.
As one politician recently said, ‘There are only so many times you can say that this is a coincidence’. He is right.
We do hope now that similar meetings for families with injured girls can be arranged with Jane Ellison, Minister for Public Health. This would give the families the opportunity to share their experiences also with the Government Health Team. The Shadow Health Team treated our families with great courtesy and with compassion and it would be excellent if both Health Teams could discuss this issue amongst themselves as this is a national issue and one to be taken seriously.
Article in it’s entirety, compliments of SaneVax.org