The observations of Karen Sullivan Sibert, MD a Los Angeles anesthesiologist, writer, and mother.
We guard the privacy of patients in my hospital zealously—we take care of a lot of celebrities since we’re right in the shadow of Beverly Hills. And of course we live in terror of HIPAA violations, those federally mandated HHS rules that protect individually identifiable healthcare information and could bring down “civil money penalties” upon us if we don’t keep our patients’ medical records strictly confidential.
But for healthcare workers—physicians, nurses, technicians, even medical supply vendors—in LA County, the usual privacy rules don’t apply any more. Now everybody gets to know at least some of our medical history: whether or not we’ve been vaccinated against influenza….
I had seen many Gardasil commercials on television and wanted to be ‘one less girl’ affected by cervical cancer. My doctor said I needed the HPV vaccine and I trusted the information I was given. I believed the vaccine was important for my health. I chose to get vaccinated.
I was not told that regular pap smears were an effective way to detect abnormal cells which could be treated before they developed into cervical cancer. I was not told the vast majority of HPV infections would clear up on their own with no health consequences. I was not given adequate information about the adverse reactions that could occur after Gardasil. I had never taken the time to research Gardasil, or any other vaccines. I believed vaccines were simply a part of the ‘healthcare’ system; a system I trusted.
I did not know vaccinating while your immune system was compromised could exacerbate the risks of adverse vaccine reactions. My doctors didn’t warn me. I wish I had known then what I know now.
My Health before Gardasil
I have been dealing with spinal issues and pain since I was a teenager. Nevertheless, I worked nearly full time at a physically demanding job and attended classes part time. In October of 2010, I had another injury that put me out of work. Because of this injury, I was prescribed heavy doses of muscle relaxers by my doctor. I had been taking those medications for six months. The muscle relaxers were causing gastrointestinal (GI) complications in my body, exacerbating GI issues I already had. So, I weaned myself off the medications a couple weeks before my upcoming OB/GYN checkup. I thought this appointment would be beneficial, and I was happy to be off the muscle relaxers two weeks prior. I was hoping to keep what small progress I had going.
My First Gardasil Injection
On January 29th, 2011, at 23 years old, I went for my Gynecological check-up with my fiancé to discuss birth control pills and the HPV vaccine. Trusting my doctor’s advice, I got my first injection of Gardasil that day.
Within the first few days and for the week after the Gardasil shot, I was bedridden, sick with what we thought was a bad flu. It was also possible I was having a reaction from the muscle relaxer withdrawal or the side effects of my newly prescribed birth control pills. I stopped taking the birth control pills after eight days and my symptoms worsened.
My mother and fiancé remember the physical changes when I wasn’t feeling well, but those few days after Gardasil have blurred together for me. I was so sick. During the days, weeks and months to come, I experienced the worst nausea, weakness, vomiting, and most severe pain in every crevice of my stomach and body that I have ever felt in my life. Even the other stomach sensitivities and spinal issues I had experienced previously absolutely paled in comparison to what happened to me after getting Gardasil.
The Doctors
We went to every doctor appointment and tested everything we possibly could. The tests kept coming back ‘normal’. (Ironically, they never tested for metal poisoning, which I expressed symptoms of. If any doctor would have known those symptoms, I had nearly all of them, perhaps I wouldn’t have suffered for so long.) None of the doctors said there could be any connection with Gardasil. In fact, most told us just the opposite; that my symptoms were definitely not caused by Gardasil. It was not until blood tests taken outside of my doctor’s office nine months later that we discovered the toxic stress, deadly amount of candida (yeast), metal poisoning and other toxins were filtering through my bloodstream. (Gardasil ingredients included; we finally connected it with certainty here after finally doing research online. We were overwhelmed with the side effects we read about, especially how similar other girls’ adverse reactions were in comparison to my own. ) Within a month of my only Gardasil vaccine I was a completely changed, debilitated human being.
The Pain and Nausea
During this period of many months, for twenty four hours a day, every moment of my life, I was nauseas, sick to my stomach and alternating puking. I could not drink water or eat anything without getting sick. Digesting anything was extremely painful and my stomach and body hurt excruciatingly. This was more pain and ongoing debilitating symptoms than I have ever experienced. It hurt and was very difficult to move, to walk or to do anything I could not even wear jeans around my waist for seven months because of how painful my stomach felt. I discovered new levels of dizziness and came close to passing out many times upon standing. I was losing weight rapidly, up to 15 pounds a month, with limited activity.
Gardasil: Before and After
Left: me in December 2010, one month before Gardasil. Right: a year and a half later, July 2012 after the extreme weight loss post Gardasil.
I tried to focus and meditate healing into my body to counteract what was happening. I lost 100 pounds within that first year and a half. My diastolic blood pressure dropped to the 50′s/40′s. It used to be consistently around 120′s/60-70′s. My hair fell out at the rate of my weight loss – quickly.
My tongue turned a grey black color in the center; my eyes turned a slight yellow. The acupuncturist, whom I was seeing before Gardasil, was documenting my progressive decline in health throughout these early months after my injection. My liver, spleen, kidneys, gallbladder, pancreas, and intestines were not functioning properly and under severe stress.
I went to the hospital once for the pain in my right side and stomach, and was given morphine, pain pills and sent home without an answer.
The most challenging and embarrassing issues were the gastrointestinal problems, which were horrifying on their own. Every time I had to use the restroom, it made me more ill than I already felt. The pain I experienced is something I will never forget. The pain in my stomach and body was disorientating every day. It physically hurt everywhere, my brain, mind and body felt foggy and deprived of energy and focus. I struggled to focus, verbalize my feelings, anxiety or frustrations because I felt so toxic and constantly overwhelmed within my own body. I was in more pain, more exhausted and more fatigued than I had ever felt. It was often overwhelming, especially trying to sleep with comfort or ease.
Meanwhile through all of this, I was told by my doctors that I had Irritable Bowel Syndrome (IBS) and to go on a whole grain diet. That was the only advice they had for us, after all my symptoms, IBS. We knew we needed other help and resources.
Family Support
My family focused all of their efforts on helping me any way they could. I was already seeing an acupuncturist outside of my insurance every week and she was documenting my progressing issues as time went on.
We bought vitamins, herbs, protein powders, digestive enzymes, probiotics, and fiber supplements to treat IBS issues. We began the first of many dramatic diet changes to facilitate gut healing.
After months of using these products, they were helping on a small scale by not making things feel worse, with some slight benefits. The nausea and pain were still constant. My back and whole body were amongst the most excruciating pains and because of the pain, my mobility, energy and strength were limited.
As the months went by, I became further immobilized. I walked as much as I was able. I tried swimming during the summer, but it exacerbated my pain greatly. My physical therapist told me, “This was as good as I was going to get.”
We decided to go somewhere else after that.
Out of Desperation
We were at our tip of desperation after I returned from a two day trip with my fiancé. We went out of town to see friends. It was traveling, something I hadn’t done during this year of many changes. We were trying to make it work even with my health complications.
It was wonderful seeing my friends, but my body could not recover from exhaustion after returning. We sought additional help.
The physicians we saw during this time had not helped, many would not help and denied my symptoms. It was my acupuncturist, who stuck with us and tried to heal me. She gave me the name of a chiropractor in the area.
It was worth a try.
Chiropractic Health
One of our biggest blessings through this chaos was finding chiropractic care and meeting my chiropractor, Dr. McKillican. He recognized the crisis my health and nervous system were in and was the first sincere and genuine doctor that strived to help us.
A chiropractor was not on any of my insurance or among the recommendations suggested to me, ever. In fact, I was advised to stay away from them earlier in life. The fifteen minute drive to their office, walking in and sitting down was excruciating, and with how my insides felt, I was deteriorating every day. We knew there, though, we had found a life-long missing link for health and healing. The adjustments I have had and which I am still continuing to have, have improved my health and lifestyle enormously.
I know with my whole being that chiropractic saved my life, especially during this crucial time of debilitating disease and sickness. I have been getting weekly adjustments for nearly two years, beginning seven months after getting Gardasil. Chiropractic adjustments have made significant and dramatic improvements in healing and strengthening my nervous system and body. Regular adjustments work on our nervous system to remove nerve interference within us and to promote the body’s natural ability to heal itself.
Vital Hematology and Nutrition
Nine months after Gardasil, I worked with a vital hematologist to detoxify my body naturally. We used a focused diet that included: juicing specific veggies, fruits, herbs, multiple vitamins, digestive enzymes, colloidal silver, olive leaf extract, glutathione, aloe vera juice. This regime greatly helped with my unbearable, chronic nausea. It seems to have reduced the intensity of pain throughout my stomach. I have had significant improvements in GI health.
This past year and a half I also began working with a nutritionist to deal with the continuous mending needed to repair my GI and organ issues, adrenal dysfunction, low energy levels and fluctuations, memory, brain, cranial issues, appetite/food challenges and over all internal damages.
I am thankful beyond words for the healing I have experienced, despite the pain and many challenges I have faced post Gardasil. My body is mending at the rate it can handle. I use my energy to focus on this.
Two and a Half Years Post Gardasil
The issues I am still working on healing and mending are different two and half years after Gardasil. Now, I primarily deal with the autoimmunity changes and pain levels. These include: gastrointestinal issues, body pain, appetite dysregulation and the ability to eat enough, malabsorption of nutrients, low blood pressure and dizziness, energy, a strong sensitivity to cold temperature, smells and chemicals.
Food and my appetite can be very overwhelming sometimes. It used to bring me to tears every day, especially my lack of desire to eat. I often don’t have the desire to eat or I get full too quickly. I also get really hungry all at once, often unexpectedly and painfully. The food and appetite issues are a constant work in progress that are still very complex.
They have become somewhat easier to work with now than in the years before. I find focusing on ratios of carbs, fats and protein I need helps me, especially with my energy fluctuations. I have also eliminated foods with gluten, GMO or that are processed. I can no longer eat foods that are spicy or acidic. I eat raw organic veggies only – juiced because my GI tract cannot tolerate the un-juiced vegetables. I watch my sugar intake, including many fruits, and other foods that I am sensitive to. I eat whole foods, organic vegetables and fruits, good fats (grass fed/organic butter and coconut oil have helped immensely here) and as much healthy, grass fed, organic protein and protein shakes as my body needs to be balanced. All this has helped substantially.
My healthy lifestyle is vital to keep my progress going. There is a combined effort of balanced nutrition, vitamins, medicinal herbs, supplements, regular chiropractic adjustments, lymphatic massages, physical therapy, removing as many toxins from my environment, and adding as much movement, exercise, walking or stretching as I can.
I also use coffee enemas and drink alkalized water (and lots of it). My body now seems to be on the path it needs to recover from the atrocity that Gardasil caused.
Every day is different with pain and energy levels, but I focus on the blessings, because I know how much worse it can be. I live in chronic daily pain, with pain levels, exhaustion and auto immune changes I never experienced before Gardasil, but these experiences have humbled me deeply in life and in the lives of my loved ones.
The Support of My Family
It has taken a substantial amount of money, time and sacrifices from my extraordinary mother and fiancé to care for me post Gardasil. They help me daily with everything, especially during times when more help is physically needed. Without them, none of this progress could have been possible. I am more grateful and humbled than ever to be alive and for all the amazing, most abundant love and support of people I’m blessed to share my life with. I could not have come this far without these wonderful people.
Gardasil changed my health, my life, and family’s lives forever; physically, mentally, emotionally, and financially.
We have had to educate ourselves about health in ways we never did before. I have a humbled appreciation to be alive after how ill I was nearly three years ago. We have learned to educate, read, and research what we put into our bodies.
We encourage everyone we know to do their own research on everything that is put into their body, especially through injection. The HPV vaccine adverse reactions will not stop until these vaccines do.
What I can give and share with others through this experience is the truth, my experiences, and the real facts and statistics regarding Gardasil. I plan to do this until this vaccine exists no more.
Thank you Nicole for your example of perseverance, humility and perspective. I hope your story travels far and many others receive your knowledge and insight. You have inspired me with your triumphant spirit. Here’s a little song of how I envision your influence on others. Thank you for your strength.
The SaneVax team is pleased to announce an opportunity for Gardasil and Cervarix HPV vaccine recipients and their families to help provide data regarding HPV vaccines’ risk versus benefit profile. The study is being conducted by an independent scientist, Dr. Chandler Marrs, and hosted on her website, Hormones Matter TM. The purpose of this study is to delineate the range, frequency and severity of adverse events as well as determine which, if any pre-existing conditions predispose one to adverse reactions. As now the vaccine has been on the market for several years, the study also looks at the longer-term side-effects and adverse events.
Whether your experience with Gardasil or Cervarix has been good, bad, or ugly, the SaneVax team encourages you to take a few minutes to complete the Gardasil Cervarix HPV Vaccine Survey. Please, help provide the information people need in order to make an informed choice when it comes to HPV vaccines. Help provide accurate data to those medical professionals who prescribe HPV vaccines.
Hormones MatterTM is a health education and direct-to-patient research community, committed to giving women the information they need to make informed medical decisions. The Gardasil Cervarix HPV Vaccine Survey is the third, in what Dr. Marrs hopes will be a long line of research projects tackling the underserved areas of women’s health. As Dr. Marrs tells her story:
I am an independent scientist, a fierce women’s health advocate and a mom. I have background in women’s health research, specifically the role of hormones in various conditions. My passions are research, diagnostics and health education. Over the last year, I developed a health site called Hormones Matter. There we cover all-manner of health related topics, even a little health policy, politics and humor. We are totally unfunded and operate purely on the passion of volunteers. I also have a company called Lucine Biotech and an organization called Lucine Women, currently unfunded as well, that will one-day offer lab based research opportunities and develop diagnostics in critical areas of women’s health.
Undeterred by the lack of funding, I decided that I would no longer wait for funding to conduct the research that needed to be completed. It was time to bring more data into the field of women’s health. About three months ago, I began conducting online research. I began with an oral contraceptives study looking at the off-label uses of oral contraceptives, along with side-effects and adverse events associated with the different formulations/brands. Phase 1 of the Oral Contraceptives Survey has over 600 respondents. The next study launched was the Hysterectomy Survey, and it has over 200 respondents so far. Last week, we launched our Gardasil Cervarix HPV Vaccine Survey. My plan is to tackle critical and ignored areas of women’s health care, one survey at a time.
As an unfunded, independent researcher, I am crowdsourcing the data collection. I rely heavily on social media and community advocates and organizations to spread the word. As a strong believer in listening to patients, I also rely heavily on the broader patient communities to inform the direction and design of the research and the even topics we cover on Hormones MatterTM. Do not hesitate to email questions, concerns, suggestions and ideas: info@hormonesmatter.com
All surveys are anonymous. They are hosted on a secure cloud site (Survey Monkey). The data reports from these surveys will be published and available to women and their physicians.
I want to thank SaneVax for supporting these efforts and to personally thank all of the survey respondents who take the time to complete this survey. Together we can improve women’s healthcare, one data point at a time. Thank you.
Thank you Dr. David Blodgett, you are a Hero among us.
By kirsten stewart | The Salt Lake Tribune
First Published Dec 06 2013 01:01 am • Last Updated Dec 06 2013 08:27 p
Citing low demand, high costs — and questioning the benefits, Utah’s Southwest Public Department of Health does not stock or recommend Gardasil, the vaccine against HPV, the cancer-causing human papilloma virus.
The decision to exclude the vaccine from its public health clinics in Beaver, Iron, Garfield, Kane and Washington counties was made years ago, not by the area’s Board of Health, but by the agency’s director, physician David Blodgett.
Demand for Gardasil, or the HPV vaccine, varies across Utah. The vaccine offers the best protection to girls and boys who receive all three doses by age 11 or 12, in time to develop immunity before they become sexually active, federal health officials say.
10.9 percent of youth between ages 12 and 17 had received one dose of the three-dose vaccine as of 2012; 6.7 percent had received two doses and 4.2 percent had received three doses.
Salt Lake County Health Department
17 percent of youth between ages 12 and 17 years of age had received one dose of the three-dose vaccine; 11.1 percent had received two doses; and 7.3 percent had received three doses.
“The backlash and sentiment against it was strong enough that there’s no reason to go there,” Blodgett explained. “No one wants it and it’s too expensive when we’re not funded to provide it.”
But in light of Utah’s dismal HPV vaccination rate, Blodgett’s decision is stirring new debate in public health circles.
The vaccine isn’t mandated in Utah. But the Utah Department of Health has been recommending it for preteen girls since 2006, and for boys since 2011.
At 42 percent, Utahranks lowest in the nationfor completion of the three-injection series among girls who start it. The national rate is 71 percent, according to the National Immunization Survey. There isn’t enough data on boys to publish.
Reasons for the slow uptake are varied, including concerns that giving the vaccine at such a young age, by 11 or 12, is a license to be promiscuous — which research has disputed, said William Cosgrove, a pediatrician in Murray and a member of the Utah Scientific Immunization Advisory Committee.
For a senior health official to downplay the benefits of a life-saving vaccine is “highly unethical,” said Cosgrove.
Gardasil is safe and more than 95 percent effective at preventing four sexually transmitted viruses responsible for 70 percent of cervical cancer and 90 percent of genital warts, he said. It’s also proven effective at preventing throat, penile and anal cancers.
“Adolescents face an 80 percent chance of being infected by one or more of these viruses,” said Cosgrove.
The three-shot series can retail for $360, but is fully covered by private insurance and provided free of charge to low-income families — and public health clinics — through the federal Vaccines for Children program.
“To be dissuaded by cost issues, or to not stock the vaccine due to low public demand, is disingenuous, especially for someone with responsibilities to protect the public,” said Cosgrove. “I believe the real medical issues here are clouded by a moralistic belief system that precludes any frank discussion about sexuality in adolescents.”
Blodgett cites other problems with Gardasil, namely that it was fast-tracked through the Food and Drug Administration (FDA) and a belief that its benefits were oversold by drug maker Merck.
“The science wasn’t good… We had physicians in our community arguing that we not make it available,” said Blodgett.
HPV is “absolutely a risk for cervical cancer,” but it’s not the only risk, he said, arguing the vaccine cuts risk by 17 percent. Cancers caused by HPV are extremely rare and immunization comes with no guarantee for long-term protection; women are still supposed to get regular Pap smears to test for the virus, he said.
Weighed against the vaccine’s risks, “the public isn’t buying it,” he contends. “It’s eroding public trust in immunization programs.”
TriCounty Health Department, spanning Daggett, Duchesne and Uintah counties, makes the vaccine available only with a doctor’s prescription.
“It’s a complicated vaccine that requires discussion about [sexual health] and a physical exam and follow-up visits with a doctor,” said the agency’s director, Joseph Shaffer. “My feeling is that’s better held in the physician’s office than here at the health department.”
Fear that Gardasil is dangerous hasn’t been eased by the FDA’s assurances. The agency approved and monitors the drug and says its safety profile matches those of other vaccines.
In response to the ensuing firestorm of criticism the show generated, Katie Couric invited Dr. Anne Schuchat, Assistant Surgeon General and Director of the CDC’s National Center for Immunization and Respiratory Diseases, to do a segment for Friday’s show in order to “make sure people understand the facts about this vaccine and human papillomavirus (HPV).”
Thankfully Norma spelled the details out for us. I happen to know, Norma cares deeply for the many girls whose journey she has shared and has researched this topic in depth. As for those girls I want them to know so many care about you and keep you in their prayers. A phrase from one of Faith Hills songs comes to mind.
“There will come a day”
It’s not easy Trying to understand How the world can be so cold Stealing the souls of man Cloudy skies rain down On all your dreams You wrestle with the fear and doubt Sometimes it’s hard, but you gotta believe…
Here’s a live concert of Faith Hill sharing this beautiful song with us. Hopefully, this can replace the inexcusable interview above.
Dr. Schuchat’s answers to Katie Couric’s questions can be viewed in the video above, or on HPV Vaccine Conversation Continued. During the interview Dr. Schuchat was asked about the safety of HPV vaccines, she stated:
“As the leader of the CDC Immunization Program, I am really committed to a very strong safety monitoring system. What I can say is more than 57 million doses have been used and with all the tests and systems that we track, we aren’t finding any concerning problems.”
Really, Dr. Schuchat – No concerning problems?
According to the CDC, VAERS data are monitored to:
Detect new, unusual, or rare vaccine adverse events
Monitor increases in known adverse events
Identify potential patient risk factors for particular types of adverse events
Identify vaccine lots with increased numbers or types of reported adverse events
Assess the safety of newly licensed vaccines
Ostensibly, the Vaccine Adverse Event Reporting System (VAERS) is the first line of defense when monitoring vaccine safety. Despite the obvious limitations of drawing concrete conclusions from VAERS data, it does provide an excellent tool for recognizing potential safety signals, red flags if you will, when looking at a specific vaccine’s safety profile.
This article will look at a few items which would raise red flags for the average medical consumer. Perhaps Dr. Schuchat can explain why they are not ‘concerning problems’ for the leader of the CDC Immunization Program.
According to the Rare Diseases Act of 2002, any disease or condition that affects less than 200,000 people in the United States is classified as a rare disease. There are currently more than 6,000 known rare diseases. One could safely assume that if one or more of these rare diseases began to show up in the VAERS database with any regularity it would certainly constitute a safety signal – a signal demanding further investigation.
Let’s take a look at a few examples of VAERS data that should at the very least raise a few eyebrows.
HPV Vaccines and ADEM
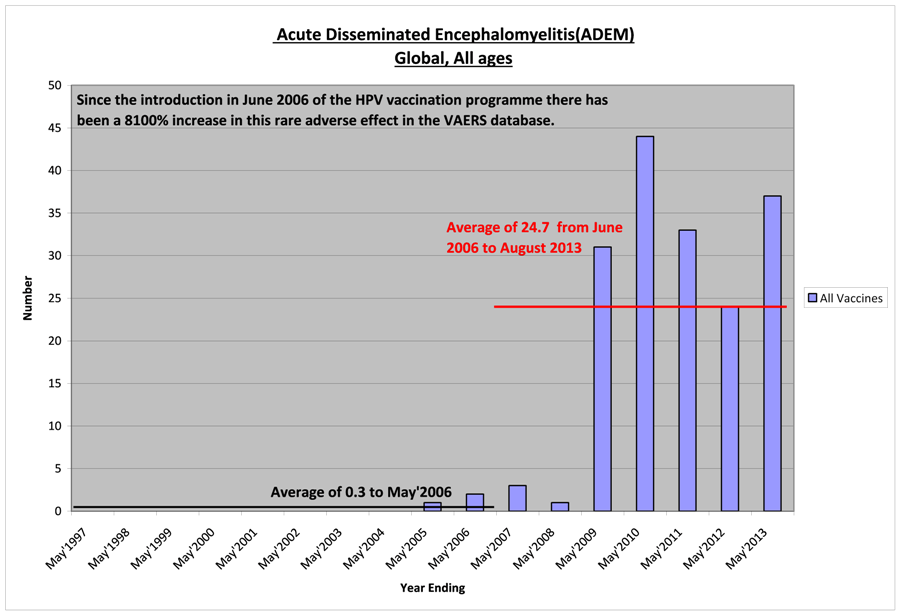
According to the NIH, National Institute of Health, acute disseminated encephalomyelitis (ADEM) is characterized by a brief but widespread attack of inflammation in the brain and spinal cord that damages myelin – the protective covering of nerve fibers. ADEM often follows viral or bacterial infections, or less often, vaccination for measles, mumps, or rubella.
In other words, ADEM is a known side effect of some vaccines. It is listed as a rare disease in both the United States and Europe. Examine the following chart showing the VAERS reports of ADEM after all vaccines used in the United States each year from May 1997 through May 2013.
One would think an 8,100% average per anum increase in reports of this rare condition after the introduction of HPV vaccines would be a huge red flag. Apparently, that is not the case for Dr. Schuchat despite the fact that ADEM is a known adverse effect of some vaccines.
HPV Vaccines and POTS
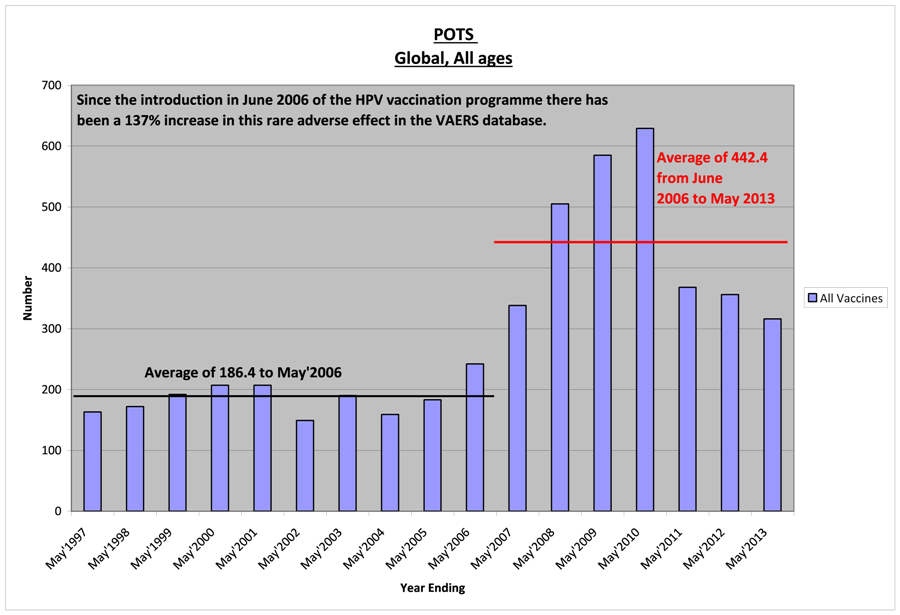
Postural orthostatic tachycardia syndrome (POTS)is one of a group of rare disorders that have orthostatic intolerance (OI) as their primary symptom (when an excessively reduced volume of blood returns to the heart after an individual stands up from a lying down position). In POTS, orthostatic intolerance causes lightheadedness or fainting, and there is also a rapid increase in heartbeat.
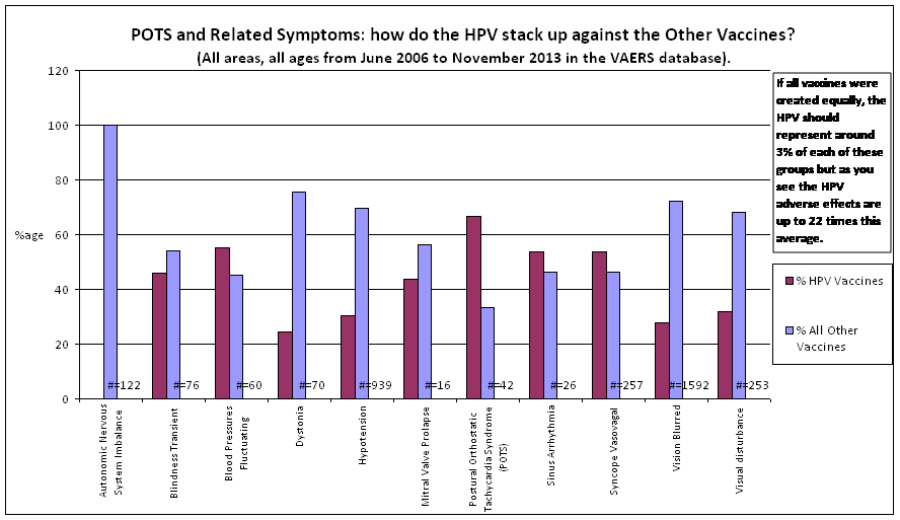
The following chart shows VAERS reports of POTS and related symptoms after HPV vaccines compared to the number of reports filed after all other FDA approved vaccines.
There are over 80 vaccines FDA approved for use in the United States. If all vaccines were equally safe, HPV vaccines should account for around 3% of the total reports filed with VAERS. As you can clearly see, depending upon the symptom, HPV vaccines account for a disproportionate percentage of the reports filed pertaining to POTS and related symptoms. What is wrong with this picture?
Still – no ‘concerning problems’ Dr. Schuchat? Not with an average increase of 137% in reports filed per year?
HPV Vaccines and ITP
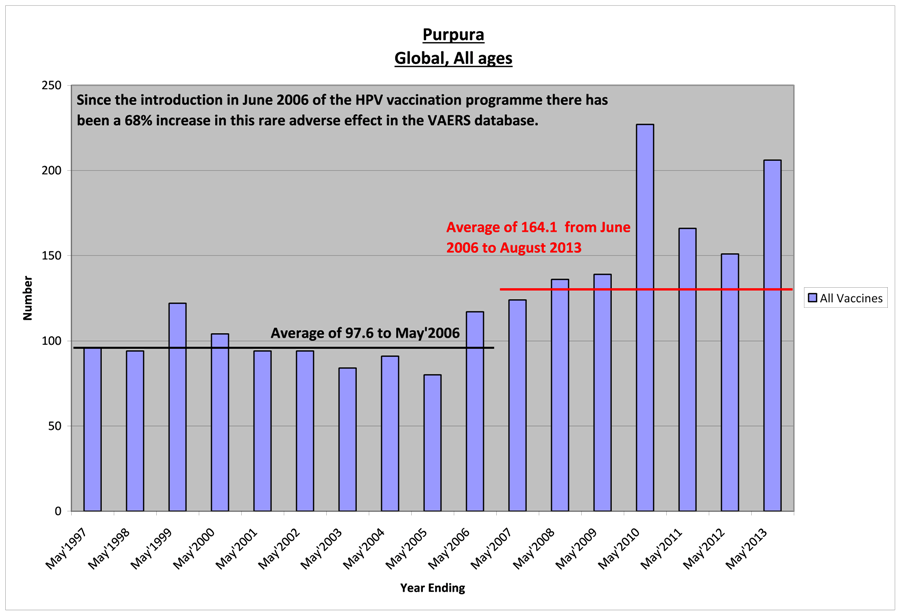
Idiopathic thrombocytopenic purpura (ITP) occurs when immune system cells produce antibodies that destroy platelets, which are necessary for normal blood clotting. The antibodies attach to the platelets. The spleen destroys the platelets that carry the antibodies.
The chart below illustrates the average number of reports of purpura on an annual basis for all vaccines listed in the VAERS database. There has been a 68% increase in the average number of purpura cases reported annually since the introduction of HPV vaccines in 2006.
Seriously, Dr. Schuchat, wouldn’t this fall under the heading of potential unusual vaccine adverse events which the VAERS system is designed to alert the members of your staff to investigate?
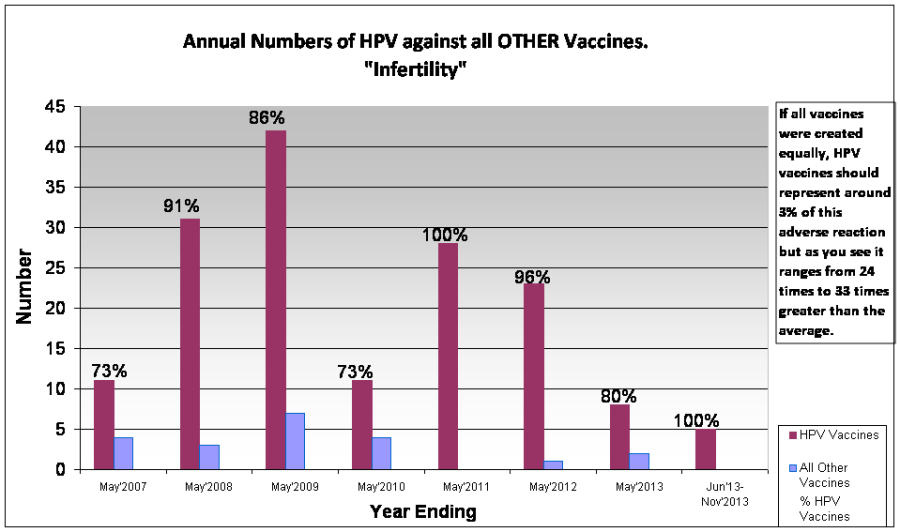
HPV Vaccines and Infertility
Infertility in the United States is no small problem. The CDC estimates that 10.9% of women ages 15 to 44 experience fertility problems. This estimate was made from data collected from 2006-2010. Since this is not a rare disorder, one would think that any signal which indicated a tendency to exacerbate the problem would be of particular concern.
OK, the chart above shows a substantial increase of the reports of fertility problems, a 790% increase in the annual average to be exact beginning in 2007. What could have caused such an increase? Does it have anything to do with the introduction of HPV vaccines in mid-2006?
Let’s compare the percentage of infertility reports after HPV vaccines to infertility problems reported after all other vaccines in the VAERS database from May 2007 to November 2013.
Dr. Schuchat, how can 2 vaccines, Gardasil and Cervarix, account for such a large percentage of infertility reports to VAERS for such an extended period of time without being a concern?
One Final Chart
Once again, Dr. Schuchat, how can two vaccines account for such a large percentage of the VAERS database? Why is this not a matter of concern?
Perhaps the mission statement for the National Center for Immunization and Respiratory Illness says it all:
“The mission of the National Center for Immunization and Respiratory Diseases (NCIRD) is the prevention of disease, disability, and death through immunization and by control of respiratory and related diseases.”
The amount of disease, disability, and death potentially caused by Gardasil and Cervarix are obviously not a ‘concerning problem’ for those who are supposed to be monitoring HPV vaccine safety at the CDC.
Thank you, Dr. Schuchat, for making that perfectly clear to medical consumers in the United States and around the world.
A printable copy is attached for those who wish to distribute it – or perhaps send to the CDC or political representatives to ask them to explain why no red flags have been raised when it comes to the question of HPV vaccine safety.
Kirstie was only 12 years old when she was diagnosed with a rare disorder for which there is no known cure, Idiopathic Thrombocytopenic Purpura (ITP). This happened just a little over a month after her second injection of Gardasil. She will live with this disorder for the rest of her life. Unfortunately, she is not alone.
Gardasil and Cervarix are two of the 76 FDA approved vaccines included in the VAERS (Vaccine Adverse Event Reporting System) database. Since Gardasil was approved for use in the United States, there have been 694 reports of ITP after vaccine administration. 127 of these reports occurred after HPV vaccines. If all vaccines carried equal risk, there should only be 18 reports of Idiopathic Thrombocytopenic Purpura after HPV vaccine use. Why are reports of ITP after Gardasil and Cervarix seven times that amount?
How rare is ITP?
When disease incidence rates are quoted, it is almost always in the context of number of cases per 100,000 people. This is not the case with ITP.
United States – adults – 66 cases per 1,000,000 per year
United States – children – 50 cases per 1,000,000 per year
Denmark and England – 10 to 40 cases per 1,000,000 per year
Kuwait – 125 cases per 1,000,000 per year
Idiopathic thrombocytopenic purpura is such a rare disorder that a diagnosis is rendered only after all other possible conditions that could cause purpura have been eliminated. This is called a ‘diagnosis of exclusion’. How many young people are living with undiagnosed ITP after HPV vaccine administration?
What is ITP?
Idiopathic simply means ‘of unknown origin.’ Frequently the word ‘immune’ is substituted for ‘idiopathic’ when referring to ITP because of the antibodies generated to specific platelet membrane proteins that cause the person’s immune system to attack their own platelets.
Thrombocytopenia is the medical term for a low blood platelet count. Platelets (thrombocytes) are minute, disk shaped particles in the blood that promote clotting. When an injury causes a blood vessel to break, the platelets are activated causing them to become spiny. The resulting ‘spines’ allow them to stick to each other and the broken blood vessel walls to begin the clotting process. The normal amount of platelets circulating in a person’s blood ranges from 150,000 to 450,000 per micro-liter. When the blood platelet count falls below 20,000 the thrombocytopenia can cause excessive internal bleeding.
Purpura refers to purple-colored spots and patches that occur on the skin, organs, and in mucus membranes, including the lining of the mouth. Purpura is caused by internal bleeding from small blood vessels.
In short, idiopathic thrombocytopenic purpura is an autoimmune disorder caused by immunoglobulin G (IgG) auto-antibodies on the platelet surface. The number of circulating platelets is reduced due to increased destruction resulting in internal bleeding of varying degrees. ITP in children most commonly occurs following an infection, or occasionally following immunisation. Acute (sudden onset) ITP often resolves spontaneously within a few months. When ITP persists longer than 6 months without specific cause, the condition is considered chronic.
What are the symptoms of ITP?
Simply having a low platelet count does not cause symptoms. However, the bleeding that a low platelet count can cause may have the following signs:
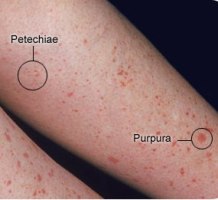
Pinpoint red spots on the skin, often found in groups that may look like a rash, caused by bleeding under the skin.
Petechiae-Purpura
These spots are called petechiae (see photo on the right).
Bruising or purplish areas (purpura) on the skin or mucous membranes caused by bleeding under the skin. (photo on the right)
More excessive bleeding can cause hematomas. A hematoma is a collection of clotted or partially clotted blood under the skin that feels like a lump. (photo lower right)
Nosebleeds, bleeding from the gums or excessive bleeding after injury.
Menstrual bleeding that is heavier than usual.
Some people experience untoward, otherwise unexplained fatigue when their platelet count is under 10,000/microl.
Hemorrhage is the most serious potential complication, intracranial (within the skull) being the most significant. (Note: the risk for major bleeding in otherwise healthy people is great only when the platelet count is less than 10,000/microl.)
Sudden severe headaches, seizures with no previous history of seizures, weakness in arm(s) or leg(s), nausea or vomiting, decreased alertness, lethargy, changes in vision, tingling or numbness, difficulty speaking or understanding speech, difficulty swallowing, difficulty reading or writing, loss of fine motor skills (such as hand trembling), loss of coordination, loss of balance, abnormal sense of taste, or loss of consciousness. (Note: many of these symptoms are often caused by other conditions.)
A diagnosis of ITP is at the very least a life changing event. Worst case scenario, it can be life threatening. Kirstie from Lima NY, now 18 years of age, is one of the lucky ones. Her diagnosis of ITP after Gardasil changed her life, but she made the most of those changes. There are others who may not have been so fortunate.
18.5% of the ITP reports in the VAERS database since the time Gardasil and Cervarix were approved for use occurred after HPV vaccinations. There are at least 126 families whose lives have been changed, perhaps forever. No one knows how many others are either undiagnosed or unreported.
Admittedly, a VAERS report does not prove causation. The problem with that line of thinking is that cause will never be established if no one looks for it.
What can you do?
Do some research if you are a considering HPV vaccination. Understand the potential risks associated with Gardasil and Cervarix as well as the potential benefits. Decide for yourself whether the potential benefits outweigh the potential risks. No one knows your family’s medical history better than you.
If you have been vaccinated with either Gardasil or Cervarix, be aware that ITP is a possibility. Don’t panic, simply be vigilant. Talk to your medical provider if you are experiencing unusual bruising or unexplained rashes.
If you are a medical professional, consider the possibility of ITP when examining patients who exhibit unexplained purpura after administration of HPV vaccines.
If you are a medical consumer, contact the FDA and CDC. Ask them why such a high percentage of ITP reports in the VAERS database occurred after HPV vaccines. Ask them why two vaccines being associated with 18.5% of the ITP reports in VAERS does not raise a red flag. Ask them why they are not ordering studies to determine whether there could be a causal relationship between HPV vaccines and ITP.
Are acute disseminated encephalomyelitis (ADEM) and Guillain-Barre Syndrome (GBS) adverse reactions to HPV vaccines? Health authorities in Japan are not sure at this point, but they have chosen to apply the precautionary principle and inform medical consumers just in case.
On March 26, 2013, the Japanese Ministry of Health, Labor and Welfare informed GlaxoSmithKline they had 30 days to alter the package insert for Cervarix by adding the following to the Precautions/Adverse Reactions section:
Acute disseminated encephalomyelitis (ADEM): Acute disseminated encephalomyelitis (ADEM) may occur. In such cases, pyrexia, headache, convulsion, movement disorder, and disturbed consciousness, etc., generally occur within several days to 2 weeks after vaccination. If ADEM is suspected, diagnosis should be made by MRI etc., and appropriate measures should be taken.
Guillain-Barre syndrome: Guillain-Barre syndrome may occur. If any symptoms such as flaccid paralysis originating from the distal extremities, decreased or absent tendon reflexes, appropriate measures should be taken.
The directive was not addressed to Merck because the package insert for Gardasil already had a reference to the risks of ADEM and GBS at the time of the directive’s issuance.
The reason for this action? During the first three years of using HPV vaccines, 3 cases of ADEM and five cases of Guillain-Barre Syndrome had been reported after Cervarix injections for which a causality to the drug could not be ruled out.1
As a point of reference, there have been 31 cases of ADEM and 121 reports of Guillain-Barré Syndrome filed with the United States VAERS (vaccine adverse event reporting system) after HPV vaccinations2 during the last seven years. The FDA has made no request that these conditions be added to the package inserts. What is wrong with this picture?
How many reports of ADEM or GBS have been filed in your country after HPV vaccinations? Has your government health officials required any modifications to the HPV vaccine package inserts?
Why did Japan take this bold step?
At first glance, the Japanese ministry’s action may give the impression that they acted on their belief in the principle of informed consent.
However, Toshie Ikeda, secretary general of the Nationwide Liaison Association of Cervical Cancer Vaccine Victims and Parents in Japan and Dr. Sotaro Sato, director of the Sato Cardiovascular Internal Medicine Hospital in Osaki, Miyagi Prefecture, believe the ministry’s action requires deep analysis. Two motivations appear to be behind their move, with one outweighing the other.
They said the first possible motive is a sincere desire to make medical doctors and other intellectuals aware of the essential nature of severe adverse effects of the HPV vaccines, Gardasil and Cervarix, in order to prevent further cases of severe damage to the health of millions of teenage girls who would otherwise be administered injections of the two vaccines during coming years.
The other possibility is fear of potential lawsuitsbeing filed by the association on behalf of numerous desperate families whose beloved, previously healthy daughters have been seriously impaired, paralyzed or horribly devastated by HPV vaccinations. Japanese courts would be likely to find health bureaucrats responsible for the serious adverse effects inflicted on the girls if they did not take precautionary measures beforehand and leave some evidence that could later be used to prove they had at least tried to do something to block the further spread of health impairments to upcoming generations of teenage girls. This would be a particular problem if the government moves to reinstate their recommendation of these vaccines during the current fiscal year ending on 31 March 2014, due to pressure from politicians and academics with financial ties or other links to the vaccine manufacturers, lobbying activities, and consulting ‘experts’ hired by the manufacturers.
You see, under Japanese law bureaucrats found to have neglected their duty to inform medical consumers of serious risks involved with taking medicines, vaccines and other medical products can be prosecuted and severely punished.
A high-profile precedent was established in 2008, when the Supreme Court upheld a Tokyo High Court ruling imposing a sentence of one year imprisonment on former senior ministry bureaucrat Akihito Matsumura¸ with a two-year stay, for neglecting his obligation to order pharmaceutical companies to stop selling unheated blood coagulants contaminated with the AIDS virus.
Chief Justice Yuki Furuta, of the nation’s top court, stated in the decision issued on March 3:
“Unheated blood products in this case were being used widely at the time of this (infection) incident and the products included a sizable number of products contaminated with the AIDS virus. The accused could have foreseen that if the products were used, numerous people would nearly inevitably get infected with the virus and develop the AIDS, causing many of the users to die eventually.”
Ikeda, who spearheaded the association, is currently being assisted by some of Japan’s best medical scientists, some politicians with strong morals, and intellectuals concerned about the fate of numerous teenage girls who have been victimized, or may be victimized in the future, unless the HPV vaccination policy is discontinued. She stated Saturday:
“It is still unknown which motivation was the bureaucrats’ primary concern when they demanded the revision of the package insert on March 26. The movements of the association have been closely monitored by the health ministry’s bureaucracy.”
Dr. Sato stated Friday he is also aware of the two possible implications of the directive issued by the ministry. He said:
“It is truly commendable that some conscientious bureaucrats at the ministry appear to have made serious efforts to alert relevant people with the directive and instruct pharmaceutical manufacturers to add references to a possible outbreak of ADEM and GBS to their package inserts. But, bureaucrats’ desire to avoid being held responsible by courts at a later date for neglecting their supervisory and regulatory duties; thus increasing the number of victims appears to have played a greater part in motivating the ministry to issue the directive.
The revision to the package inserts would make a meaningful difference, if a lawsuit were filed down the track. With the issuance of the directive, bureaucrats would be able to tell victims, parents and their supporters that the ministry had issued an important warning on possible adverse effects and that the victimized are therefore responsible, as they simply did not notice the reference to the risks thus included in the insert.”
Dr. Sato called attention to the coincidental dates: with the association holding the first meeting of vaccine victims and their parents on March 25 – one day before the issuance of the directive. The ministry must have been following a string of events leading to the establishment of the association for which people of good intentions joined forces to free victims from their agony and prevent the drug manufacturers, medical associations and government from producing more victims, whether unintentionally, through half-awareness and knowledge of adverse events, or due to callous indifference to possible serious consequences of HPV vaccines on girls’ health.
Dr. Sato called attention to another key dimension of the HPV vaccination issue now being faced by numerous doctors in Japan and elsewhere, when he stated:
“When a doctor sees a girl who developed various symptoms caused by ADEM or GBS following vaccination, he or she would not be able to recognize the symptoms as those resulting from ADEM or GBS unless that doctor had deep knowledge of neurological disorders or diseases. It is not easy for doctors to associate symptoms they are seeing with ADEM or GBS. In Japan, the percentage of doctors who can recognize the symptoms of girls who one day come to see them as consequences of ADEM must be less than 0.1 percent of our doctors’ population.”
Government authorities need to draw up and issue unified diagnostic criteria to help doctors recognize symptoms induced by ADEM and GBS as such and call the attention of doctors to said criteria. Most doctors who may see vaccine-ravaged girls in the future must be made familiar with the symptoms.
Dr. Sato warned:
“Merely getting drug makers to alter the package insert is not adequate to increase the awareness of doctors and medical consumers of the potential risks of these two vaccines. Unless the government makes very serious efforts to direct attention to the possible horrible adverse effects of these vaccines, it is likely many doctors will continue administering injections of the vaccines without being able to pay necessary levels of attention to the causal link between the vaccines and their adverse effects.”
Japanese politicians speak
28 March 2013, a select Committee for Health, Welfare and Labor held a special session so questions about HPV vaccines could be addressed prior to a parliamentary vote on whether to add three diseases, cervical cancer being one of them, to the list of vaccines whose cost should be fully covered by the government under the nation’s existing Preventive Vaccination Law.3
Of the 722 members of Japan’s Parliament, two voices have repeatedly questioned the sanity of universal HPV vaccinations in Japan, particularly strongly both on the parliamentary floor and via the mass media. One voice was Ms. Tomoko Hata, Member of Parliament, but not a member of the Committee for Health, Welfare and Labor. The other was that of Mrs. Eriko Yamatani, a former aide to Prime Minister Shinzo Abe. Abe’s Liberal Democratic Party toppled the leftist-dominated Democratic Party of Japan in a general election for the House of Representatives, the more powerful of Japan’s bicameral parliamentary system, only on December 16, 2012, with Abe assuming the premiership on December 26.
Ms. Hata made sure those present at the question and answer session were made aware of the following facts about HPV and cervical cancer in Japan:
The proportion of Japanese women who carry HPV types 16/18 is much lower than women in western countries. (0.5% for HPV 16 and 0.2% for HPV 18)
More than 99.1% of the carriers of human papillomavirus will not get cancer.
90% of those exposed to HPV will discharge/clear the virus in 2 years.
90% of those who develop very early signs of cervical cancer (cervical dysplasia) will recover spontaneously.
The number of serious adverse effects reported was 52 times greater after Cervarix than reports after flu vaccinations; 26 times higher after Gardasil than after flu vaccinations.
The same day, Japan’s Parliament voted to include cervical cancer in the list of vaccines that are fully subsidized by the government under the law. Hata voted against the proposed inclusion, while Yamatani and a few others abstained on the vote.
Four years earlier, on October 16, 2009, the government of Japan, which was still under the control of the leftist DPJ-led government approved the sale of Cervarix in Japan. Then, on February 1, 2011, the government began spending taxpayer money via a partial subsidy program, under which the cost of HPV vaccines was split between the central government and local prefectural governments across the nation. Under this program, the central government put up 15 billion yen under the “emergency promotion program.” After the subsidy program was put in place, the marketing of Gardasil was approved on July 1, 2011. The DPJ-led government and the health ministry jointly adopted a policy of fully subsidizing the vaccines on May 23, 2012, despite the fact they were aware of reports of outbreaks of numerous cases of adverse reactions among recipients. This was followed by a change of power last December.
Since the coalition government of Abe’s LDP and the New Komeito Party, as well as opposition parties overwhelmingly voted to start fully subsidizing HPV vaccines on March 28, 2013, the government set aside 100 billion yen for the fiscal year that started on April 1st.
Because the LDP-led government took over the health ministry’s bureaucracy, which had cooperated with the DPJ-led government, it also took over the agreement to fully subsidize HPV vaccine administration. The new administration found it difficult to correct and jettison the wrong policy while the vaccine manufacturers continued to lobby to preserve the full subsidization policy through various channels and connections with powerful political circles.
Cervical cancer vaccine victims and parents organize
Meanwhile, victims of serious adverse reactions throughout Japan organized under the Nationwide Liaison Association of Cervical Cancer Vaccine Victims and Parents. Through the collection of adverse event reports from individuals (see link to chart below[4]), they began to understand that the officially reported adverse events were merely the ‘tip of the iceberg.’
This organization is currently petitioning government health officials to:
Ban the use of HPV vaccines in their country and acknowledge HPV vaccine injuries
Establish treatment for HPV vaccine victims
Provide financial relief for HPV vaccine victims
Investigate all who have been inoculated with HPV vaccines
Include the nation’s top neurological scientist, who saw dozens of victims, in a health ministry committee on the fate of the vaccines
Japan suspends HPV vaccine recommendation
The Nationwide Liaison Association of Cervical Cancer Vaccine Victims and Parents has apparently made an impression on their government health officials.
In an unprecedented move, less than three months after pushing legislation through Parliament granting full subsidization of HPV vaccines, government officials in Japan suspended that recommendation pending the outcome of investigations into the safety of Gardasil and Cervarix.5,6
On the same day the HPV vaccine recommendation was suspended, 14 June 2013, the health ministry issued another directive to the chairman of the committee on safety of medicines at the Federation of Pharmaceutical Manufacturers’ Association of Japan in the name of Tomiko Tawaragi, Director of Safety Division, Pharmaceutical and Food Safety Bureau.7 This letter required the manufacturers of Gardasil and Cervarix to add the following to the ‘Precautions’ section of their package inserts within the next 30 days:
“Although the mechanisms of pathogenesis are unclear, severe pain which is not localized at the injection site (e.g. muscle pain, arthralgia and skin pain, etc.), numbness, weakness, etc., may occur after vaccination and these symptoms may persist for long time. Vaccine recipients and their guardians should be instructed to consult a healthcare provider who can provide appropriate medical care including making neurological and immunological differential diagnosis if any abnormalities are observed after vaccination.”
Please note, the paragraph above instructs vaccine recipients and/or their guardians to consult a physician if ANY abnormalities are observed after vaccination. Have medical consumers in your country been made aware of these possible adverse reactions?
Japan’s actions raise questions for medical consumers worldwide
1) Do your health authorities believe in the right to informed consent?
2) Will the risks associated with HPV vaccines be explained, as well as the benefits?
3) Will alternative cervical cancer preventive measures be explained?
4) Will the risk factors for developing cervical cancer be explained?
5) Do health authorities in your country understand what adverse effects are possible after HPV vaccines?
6) Are your healthcare providers trained to recognize these events as possible vaccine reactions?
7) What happens if you experience an adverse reaction to an HPV vaccine?
Think about it – if HPV vaccines are as good as they should be, all of these questions should be easy to answer. You have a right to know. It is called the right to informed consent.
What is more important to you – vaccine safety, or vaccine uptake?