Tag: world cup
Vaccinations Linked to Autism#vaccines#iBelieve#ASD
We are told repeatedly that study after study has shown vaccinations to be safe and not to be linked to autism. Just reading the vaccine inserts, you will discover that vaccines are not 100% safe – a fact that is reiterated by discussions with pediatricians. However most pediatricians would still recommend vaccinating as they feel the benefits outweigh the risks. 
Regarding all the research that has been done not linking vaccines to autism, there are actually studies that do link vaccines to autism. These studies were not funded by the pharmaceutical industry and are often dissected by those who whole-heartedly support vaccines even though the pharmaceutical studies are taken at face value.
Hepatitis B Vaccine and Autism
Prior to 1999, the Hepatitis B vaccine contained thimerosal (49.6% mercury by weight). A study was performed in 2010 to determine if vaccines containing thimerosal given prior to 1999 were linked to autism. The Journal of Toxicology and Environmental Health found that there was in fact a link….
HPV Vaccines: Time for Science#iBelieve#vaccines#HPV

By Norma Erickson
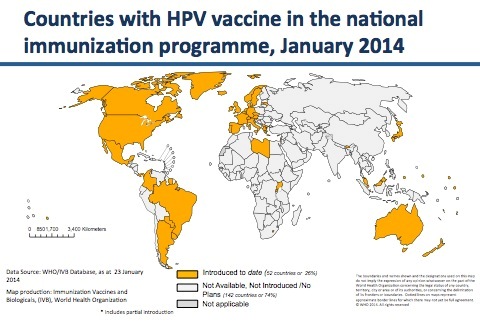
According to the World Health Organization (WHO), as of January 2014 fifty-two countries have included HPV vaccines, either Gardasil or Cervarix, in their national immunization programs. During the last five years, the SaneVax Team has been contacted by representatives from 24 of those countries who are seeking to understand the vast array of new medical conditions occurring in the wake of these programs.
 (Note: SaneVax has been contacted by multiple people in Australia, Argentina, Belgium, Canada, Colombia, Denmark, Finland, France, Germany, India, Ireland, Israel, Japan, Malaysia, Morocco, New Zealand, Norway, Peru, Scotland, Spain, Sweden, Switzerland, the United Kingdom and the United States – all requesting further information on HPV vaccines and vaccination programs.)
(Note: SaneVax has been contacted by multiple people in Australia, Argentina, Belgium, Canada, Colombia, Denmark, Finland, France, Germany, India, Ireland, Israel, Japan, Malaysia, Morocco, New Zealand, Norway, Peru, Scotland, Spain, Sweden, Switzerland, the United Kingdom and the United States – all requesting further information on HPV vaccines and vaccination programs.)
Why would so many countries contact an organization dedicated to the promotion of only safe, affordable, necessary and effective vaccines and vaccination programs in such a relatively short period of time? Let’s take a look at the science.
In 2006, when the FDA approved the first HPV vaccine (Gardasil) for cervical cancer prevention they should have known that HPV does not cause cervical cancer without other risk factors being involved. They should have known that the endpoints chosen to evaluate the efficacy of the vaccine were not sufficient to prove future cervical cancer prevention because ASCUS and CIN1/2/3 frequently resolve on their own, or can be detected by currently available tests (pap smears) and treated safely and effectively prior to progression to cervical cancer. They should have known that allowing the manufacturer to use a reactive aluminum adjuvant as a ’control solution’instead of an inert placebo could potentially mask adverse effects making the vaccine appear more safe than it actually is.
Any one of these facts should have raised questions about the practicality of utilizing HPV vaccines in any cervical cancer prevention program. Apparently the facts above were either not known, or they were ignored. Gardasil was awarded fast-track approval despite the fact there was no cervical cancer crisis in the United States. A short time later, Cervarix was approved for the same indication.
Since health officials at the FDA are apparently ignoring scientific facts medical consumers need to be aware of the science, or lack therof, behind HPV vaccines.
Does HPV cause cervical cancer?
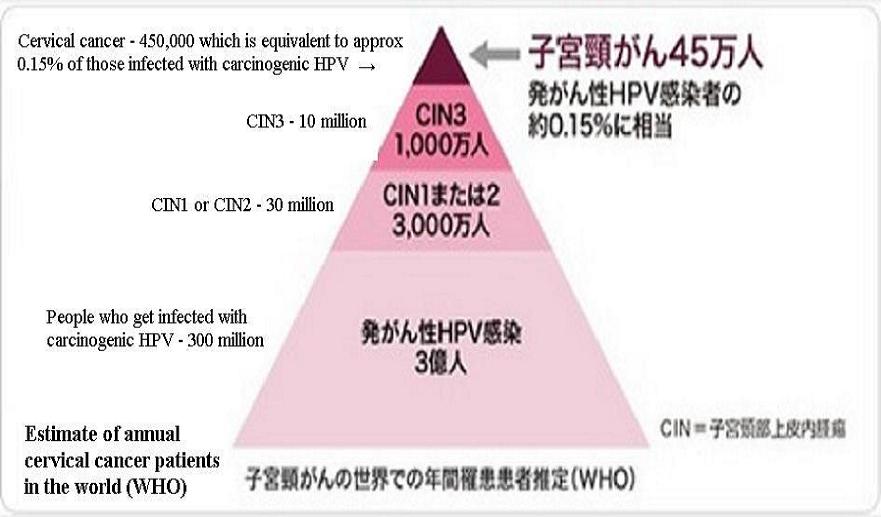 According to WHO, only 0.15% of people exposed to any high risk HPV types will ever develop cervical cancer. We do not have a publication date on the chart to the right, so let’s assume this is new knowledge, information which the FDA officials responsible for the fast-track approval of Gardasil did not have when they made the decision to approve the vaccines for cervical cancer prevention.
According to WHO, only 0.15% of people exposed to any high risk HPV types will ever develop cervical cancer. We do not have a publication date on the chart to the right, so let’s assume this is new knowledge, information which the FDA officials responsible for the fast-track approval of Gardasil did not have when they made the decision to approve the vaccines for cervical cancer prevention.
Medical consumers need to know that according to the World Health Organization 99.85% of those exposed to oncogenic types of HPV will never develop cervical cancer.
IF the FDA did not know this prior to approving HPV vaccines to ’prevent’ cervical cancer, they are most assuredly know it now. Consider the following quote from an FDA/CBER (Center for Biologics Evaluation and Research) meeting held on September 19, 2012 to discuss the use of human tumor cells in vaccine production (verify on pages 91-92 of this transcript):
“However, even tumor induction by acute oncogenic viruses requires additional oncogenic events. The best example is the Human Papillomavirus, where even infection with a high risk of Papillomavirus types is not sufficient to induce cervical cancer. Mutation in other genes and perhaps also epigenetic events are required. If a single infection-induced cervical cancer after infection with HPV, say, 16, then teenagers will be getting cervical cancer. And as we know, cervical cancer is a disease of older people”.
So, there you have it – even infection with a high risk strain of papillomavirus types is not sufficient to induce cervical cancer. Since at least September 2012, FDA officials knew infections with high-risk HPV types will not induce cancer without genetic mutations and/or other epigenetic (relating to or arising from nongenetic influences on gene expression) events occurring also.
Did this cause the FDA or CDC to re-examine the usefulness of HPV vaccines? No.
Were clinical trial endpoints valid?
Prior to the marketing push for HPV vaccines, CIN1/2/3 were known as abnormal cells – something that needed to be observed until treatment was required. Now, they are almost always referred to as ‘pre-cancerous’ lesions. This serves no purpose other than to strike fear into the heart of almost any woman on the face of the planet. The nature of the abnormal cells has not changed, simply the terminology. No mention is made of the fact that CIN1, CIN2 and often CIN3 abnormal cells revert to normal cells without medical intervention.
Not many people are aware of the fact that most CIN1 lesions go away on their own within two years. 25-50% of CIN2 lesions regress on their own within the same two year time frame. According to the International Agency for Research on Cancer (IARC), World Health Organization, the results of a pooled analysis of studies published between 1950 and 1993 indicated only 12% of CIN3 lesions progress to invasive cervical cancer.
Consider the following quote from Chapter 2 of the IARC’s COLPOSCOPY AND TREATMENT OF CERVICAL INTRAEPITHELIAL NEOPLASIA: A BEGINNER’S MANUAL states:
“Despite women’s frequent exposure to HPV, development of cervical neoplasia is uncommon. Most cervical abnormalities caused by HPV infection are unlikely to progress to high-grade CIN or cervical cancer, as most of them regress by themselves. The long time frame between initial infection and overt disease indicates that several cofactors (e.g., genetic differences, hormonal effects, micronutrient deficiencies, smoking, or chronic inflammation) may be necessary for disease progression. Spontaneous regression of CIN may also indicate that many women may not be exposed to these cofactors.”
Please note this manual was designed to teach medical and nursing personnel in developing countries where diagnostic and therapeutic expertise is not readily available. In other words, the progression from HPV exposure to potential development of cervical cancer is similar in both developing countries and developed countries. It also indicates that several cofactors (risk factors) may be needed for HPV exposure to progress to abnormal lesions, much less cervical cancer.
Surely, FDA officials were aware of the information contained in a beginner’s manual to treatment of so-called ‘precancerous’ lesions published by the World Health Organization. If not, they certainly should have been. Nevertheless, they allowed these very same abnormal cells which typically revert to normal on their own to be used to evaluate the efficacy of HPV vaccines against cervical cancer.
Medical consumers need to know, according to WHO only 1% of CIN1, 1.5% of CIN2 and 12% of CIN3 progress to invasive cervical cancer. This is in developing countries. In countries where pap smears are routinely administered the percentages should be much lower. Could using these abnormal cells as endpoints in clinical trials artificially inflate the predicted efficacy of HPV vaccines against cervical cancer? Absolutely!
Why not use a true placebo during clinical trials?
When conducting scientific experiments to evaluate a new substance, standard practice is to have at least two groups – one group using the substance being examined and the other using a placebo. This way, the scientific team can evaluate the effects and safety of the new substance by comparing both groups’ results at the end of the study.
The definition of placebo is “a substance having no pharmacological effect, but administered as a control in testing experimentally or clinically the efficacy of a biologically active preparation.”
There is no doubt about vaccines being a biologically active preparation. But, how about aluminum – one of the major ingredients in the proprietary AAHS solution which Merck was allowed to use as a control solution in the vast majority of clinical trials for Gardasil?
A quick search of PubMed, using the terms ‘aluminum toxicity human’ returns 1620 papers on studies conducted as early as 1966. If you narrow the search to ‘injected aluminum toxicity’ you come up with 116 papers published as early as 1974. Refine the search even further to ‘injected aluminum toxicity human’ and you still get 31 scientific papers published between 1979 and 2014.
It is extremely difficult to believe the FDA officials responsible for reviewing Gardasil’s application for approval did not know that aluminum compounds were potentially toxic to humans. Yet, they accepted the use of a proprietary (meaning no one knows what was included other than aluminum) AAHS aluminum adjuvant as a control solution instead of an inert placebo.
FDA officials knew, or should have known, that clinical trials conducted in this manner proved nothing other than the fact that Gardasil was no less dangerous than the new AAHS adjuvant which had never been tested for safety in humans. FDA officials ignored the fact that over 70% of all clinical trial participants reported new medical conditions after the trials. (Verify here) One can only speculate as to why this fact did not raise a huge red flag, but apparently it did not.
The FDA could certainly not use the excuse that it would be unethical to withhold vaccination from any of the clinical trial participants because there was currently no ‘comparable’ vaccine available. Why then, did they not require a real placebo?
Is the FDA ignoring new scientific evidence?
Below is a list of scientific information presented to government health officials around the world. None of the presentations below have brought forth a response from FDA officials. Please keep in mind this is by no means a complete list; it is simply a sample:
- February 2014, information presented to Japanese Government health officials by Dr. Sin Hang Lee, Director Milford Medical Laboratory, Inc. (Dr. Lee’s presentation in Tokyo)
- February and May 2014, information presented at a meeting of Japanese Senators by Lucija Tomljenovic, PhD; her and Professor Christopher Shaw presented similar data to health officials in France (Lucija Tomljenovic’s presentation in Tokyo)
- May 2014, presentation to French health officials by Christopher Exley PhD (Chris Exley’s presentation in Paris)
- December 2012, Professor Joe Cummins, Institute of Science in Society, writes DNA Contamination in HPV Vaccines.
How long are medical consumers supposed to put their faith in an agency that repeatedly ignores standard scientific methodology, not to mention scientific evidence? Medical consumers need to remember every single medication that has ever been pulled from the market was first approved ‘safe and effective’ by the FDA. Can you trust them with your life?
Remember – Research before Consent – you can’t un-vaccinate.
Spotlight on Gardasil in France#Vaccines#HPV#iBelieve
By Helen Kimball-Brooke MARH, guest author
A press conference on the Gardasil vaccine was held in Paris on Wednesday the 2nd April 2014 at the local offices of the European Parliament, a short walk from the French National Assembly. It was organised by MEP Michèle Rivasi (Vice-Chair of the Greens/European Free Alliance group) who has held meetings in the past on pharmacovigilance in Brussels and other press conferences on the aluminium salts used as adjuvants in vaccines, in Paris. Three members of EFVV (the European Forum for Vaccine Vigilance) attended the conference: myself, Françoise Joët from the French group ALIS and Dr. Françoise Berthoud, retired homeopathic paediatrician from Switzerland.

Aside from Michèle Rivasi, the speakers included the parents of two HPV-vaccine victims: 18-year-old Marie-Océane Bourguignon who after receiving two doses of Gardasil at age 15 now suffers from multiple sclerosis (MS) and Orianne Lochu, age 21, a former first-year medical student now struggling with severe macrophagic myofasciitis, an illness thought to be linked with the aluminium adjuvants in vaccines. Both HPV vaccines, Gardasil and Cervarix, contain aluminium salts. Within months of her jabs, Océane, the only French HPV vaccine victim for whom the link to the vaccine has been officially recognised by a Medicine Injury court, temporarily lost both her sight and the use of her legs after being hospitalised for what appeared to be either acute disseminated encephalomyelitis (ADEM) or multiple sclerosis.
Océane’s case was originally heard by the Bordeaux Commission de Conciliation et d’Indemnisation or Medical Accident Arbitration and Compensation Committee, set up by the Ministry of Justice with members appointed by the local Public Health Authority. As of the judgement in September 2013 she was awarded compensation amounting to 50% of her claim but given that Sanofi-Pasteur were clearly incriminated in the case and thinking of all the other victims, her parents chose to forfeit the compensation by filing charges in the criminal courts. The criminal court case is still pending.
The parents of both girls expressed anger and frustration over the way they had been treated: refusal by the medical profession to acknowledge that their daughters’ illnesses had been triggered by the vaccine, lack of support and treatment for the girls’ ailments, even suspicion and ostracism for having dared to blame the vaccine. The experience has been all the more difficult for Orianne’s parents who are medical professionals themselves: her father is an anaesthesiologist and her mother a nurse.
Océane’s lawyer, Maître Jean-Christophe Coubris, also defending over 100 other French HPV-vaccine victims, was another speaker, as was Serge Rader, a pharmacist who has done research on the widely varying prices of vaccines across Europe, and Elena Pasca, a philosopher, member of the board of Sciences Citoyennes and author of a blog called Pharmacritique, who discussed the conflicts of interest inherent in the development and marketing of these vaccines.
Others present included French medical consultants Profs. Authier and Gherardi, doing research on the aluminium salt adjuvants in vaccines at the Henri-Mondor Hospital in Créteil, a Parisian suburb, and consultant Dr. Laurent Belec, head of the virology laboratory at the Georges Pompidou European Hospital in Paris. The sudden withdrawal in 2013 of the funding for the important work of Authier and Gherardi was the topic of another press conference organised by Michèle Rivasi last year. Their funding was only re-instated after two members of the NGO victim support group E3M went on a hunger strike.

The speakers of honour however were Drs. Christopher Shaw, neurologist, and Lucija Tomljenovic, PhD, from the University of British Columbia, Canada, known for their research on Gardasil and the dangers of its adjuvants. Currently doing research with Professor Yehuda Shoenfeld in Tel Aviv, Israel, on vaccine adjuvant-induced autoimmune diseases, they spoke of the effects on the body of the aluminium in vaccines. It has been shown that aluminium migrates through the body to the brain, where it accumulates, potentially causing many adverse effects: convulsions, fainting spells, Guillain-Barré syndrome, transverse myelitis, facial paralysis, chronic fatigue syndrome, autoimmune diseases, pulmonary embolisms, macrophagic myofasciitis, pancreatitis and even death.

Dr. Tomljenovic demonstrated how these vaccines were rushed prematurely to market. In the USA, the FDA approved the vaccine very fast, reflecting, in her opinion, the flaws and incompetence which are now sadly a characteristic of the organisation. Development of cervical cancer from HPV infection is in fact very slow and 90% of HPV infections resolve of their own accord within three years. The duration of follow-up in the clinical trials was only 4.5 years for Gardasil and 8.4 years for Cervarix but given the slow growth of these cancers, at least 15 if not 20 years would really be needed to establish accurate efficacy. The manufacturers have nonetheless claimed 70% efficacy based on these short-term trials, and Sanofi-Pasteur, who market Gardasil for its manufacturer Merck, have even claimed ‘up to 100%’ efficacy while true vaccine efficacy could be as low as 16.9%.
STIKO, the German Standing Vaccine Committee’s flawed assumption that the vaccine would confer lifelong protection of 92.5% led to the decision to reimburse the HPV vaccine in Germany and incited many German doctors to recommend it. Since its introduction 7 years ago, nearly 2 million young French women between the ages of 13 and 26 have received at least one dose of Gardasil, reimbursed at 65% by the Social Security, even though its effectiveness has not yet been proven and is highly controversial. There are in fact over 100 strains of HPV but Gardasil contains only antigens from strains 6, 11, 16 and 18, considered the most oncogenic. Strains 16 and 18 are responsible for 70% of cervical cancers which is why these are the only two in Cervarix but infections with these two strains also seem to be less common in Europe. In fact, cervical cancer represents only 1.7% of all cancers in France so it is not actually a public health problem there anymore.
On the 4th of February 2014 however, President François Hollande announced that as part of his ‘Cancer Plan’, he wanted HPV vaccine uptake amongst young French women to double over the next five years. This came as an enormous shock to the parents of the 10 girls with very severe neurological complaints, who by November 2013 had already initiated legal proceedings against both Sanofi Pasteur and ANSM, the French national medicines safety authority.
To quote Dr. Tomljenovic:
‘Just as pizza-bearing cheerleader drug reps are a poor substitute for medical education, pharmaceutical lobbying is a poor substitute for well-reasoned public health policy-making….Is it ethical to put young women at risk of death or a disabling autoimmune neurodegenerative disease at a pre-adolescent age for a vaccine that has not yet prevented a single case of cervical cancer, a disease that may develop 20-30 years after exposure to HPV, when the same can be prevented with regular Pap screening which carries no risk?’
The number of HPV vaccine victims continues to grow in France and worldwide, with some countries taking a more cautious stance: Austria refused from the start to include the HPV vaccine in its vaccination schedule and during 2013, under pressure from victims, the Japanese Ministry of Health, Labour and Welfare withdrew its recommendation for the HPV vaccine. Shortly after the press conference in Paris, it was announced in Japan that instead of reinstating the HPV vaccine recommendation, the authorities would hold off for at least another year.
On the 30th March, only three days before the press conference, it was reported in French newspaper Journal du Dimanche that 420 French doctors plus nearly another 300 pharmacists, midwives and other medical professionals had signed a petition demanding a parliamentary mission to reassess Gardasil, claiming that its effectiveness is limited (only 20% according to clinical trials) and its cost exorbitant. They also fear that the vaccine may mislead women into thinking that a Pap smear, whose effectiveness has been proven, is not necessary. As of late May 2014, there were nearly 1200 signatures on the petition.
Of course a counter-petition was also launched by seven scholarly medical groups affirming the benefits of the vaccine but speaking of cost: what in fact is the actual cost of this HPV vaccine campaign in France? Mr. Rader informed us that a single dose of Gardasil costs €123.44, compared with prices ranging from €6.50 to €57 for other French vaccines, the prices of which have increased as new vaccines were introduced over the years. The three jabs required would therefore come to a whopping total cost of €370.32 per individual. The duration of protection conferred by the initial vaccination is still not known so the overall cost would increase if boosters were required. A ‘catch-up’ period could generate a cost to the French Social Security of a shocking €926 million and in subsequent years, the annual cost would be €148 million. What incites more questions however is that a single dose of Gardasil costs only €60.50 in Italy and the Rotavirus vaccine recently recommended for all new-borns by the French High Council for Public Health, costs €54.60 per dose, including tax, compared with only $1 per dose in India. Why do vaccines cost so much in France?
Pap smears, costing €15.40 each in France, remain the best and most effective way to fight cervical cancer. The speakers therefore questioned why the French government was so intent on pushing Gardasil whose effectiveness is debateable and will not be known for 15 or more years, let alone its excessive cost. An indecent communication campaign with lobbying and aggressive advertising was apparently engaged a number of years ago to promote this vaccine. The adverts played on the fears and guilt especially of mothers and in 2010, one of them was even banned for ‘lack of objectivity’ by the French Medicines Agency.
Mme. Rivasi therefore concluded the press conference with a forceful:
‘Enough is enough! It is time to demand a moratorium on this vaccine! EU member states must stop recommending this vaccine until more studies are conducted on Gardasil, its effectiveness and its dangers.’

Less than two months later, her efforts seemed finally to be having some effect: on the 22nd May, under pressure from victim support groups, primarily E3M, an NGO supporting patients with macrophagic myofasciitis, two colloquia with round-table debates open to the public and in the presence of the press, television and even French Health Minister Marisol Touraine, were organised at the French National Assembly: one in the morning by E3M and facilitated by journalist Viginie Belle, the other in the afternoon by Office parlementaire des choix scientifiques et technologiques (Opecst, similar to our House of Commons Science and Technology Committee).
A fair number of the speakers from the April press conference (Gherardi, Authier, Shoenfeld, Orianne Lochu’s mother, Tomljenovic, Belec, Rivasi) took part, alongside representatives from Sanofi-Pasteur, GSK, the French government and other scientists promoting vaccines. Pro-caution and pro-choice scientists also included our own Prof. Christopher Exley from Keele University, Dr. Lluis Lujan, veterinary pathologist from the University of Zaragoza in Spain and Prof. Michel Georget, French biologist and author of books on the adverse effects of vaccines.
Topics of the four round-table debates: 1) Aluminium: Adjuvant under Scrutiny. 2) HPV Vaccine: Time to Exercise Caution, in the morning. Then in the afternoon: 1) The Safety and Efficacy of Aluminium Vaccine Adjuvants. 2.a) Is a Moratorium Appropriate? 2.b) Are there Alternative Vaccine Adjuvants?
For those who speak French, these debates can be viewed here: http://videos.assemblee-nationale.fr/video.5464. Compared with our House of Commons Science and Technology Committee’s Evidence Check into Homeopathy in 2009, this series of debates seemed far more balanced! The focus in France seems at present to be only on aluminium, which may not be the only issue but time will tell as to where it takes the whole French and European vaccine debate.
Knowing that the French Health Minister attended these colloquia and is therefore now fully aware of the latest research on the damage caused by aluminium adjuvants and the Gardasil vaccine, it came as a shock when instead of calling for a moratorium she later reaffirmed the French government’s intent to vaccinate all young French women with this vaccine. Yet another debate was then organised on the 23rd of June by a group of galvanised GPs from La Réunion island, one of France’s overseas departments. The thrust of this series of medical and statistical presentations, again hosted by Michèle Rivasi, was that HPV vaccination is not needed to prevent cervical cancer, is excessively costly and the whole vaccine development and marketing process is fraught with conflicts of interest. Gardasil is clearly a hot topic in France with articles, blogs, petitions and debates appearing frequently. The doctors, researchers, support groups and victims behind these are not about to give up the fight for both a moratorium on Gardasil and aluminium-free vaccines in general.
Remember that in the USA and the UK, HPV and other vaccine victims are fortunate to have SaneVax (http://www.sanevax.org) who in addition to providing the necessary information for making an informed choice, can locate appropriate medical/legal assistance in the event of an adverse event post-vaccination.
Since the April press conference, the EFVV has prepared a Manifesto in English, French, Spanish, Italian, German, Dutch and Slovenian (other languages possibly to follow), demanding the abolition of mandatory vaccination in the EU (see http://www.efvv.eu). The plan is to launch a petition based on this Manifesto and a delegation of EFVV members will be meeting with Michèle Rivasi in September to discuss the best way to utilise these documents and submit their demands to the European Parliament. Watch this space, both in France and Europe-wide.
(Note: This article was originally written for Homeopathy in Practice, the journal of the Alliance of Registered Homeopaths in the UK but, with kind permission of HIP, is appearing here first.)
UK: Parliamentary meeting with families of girls injured by HPV vaccines#iBelieve#HPV#Vaccines
By Freda Birrell
We would like to thank Luciana Berger, MP Shadow Minister for Public Health, her Parliamentary Assistant Kat Thompson, The Countess of Mar from the House of Lords, Pat McFadden, MP, Joe Benton, MP, Mary Creagh, MP and Tom Fieldhouse, researcher in the office of Oliver Letwin, MP for taking the time to meet the parents and girls who had an adverse reaction to the HPV vaccines.
From the presentations given we would like to highlight a few very disturbing points which we hope Ms Berger will take on board and ask relevant questions. The points made are not unique to this group of families from the United Kingdom. They are the same for many families around the world.
- Serious loss of education and the opportunity to interact with their peers socially;
- Young girls’ mental health being questioned without justification; psychiatric care being promoted time and time again;
- Threatening behaviour towards families by health care officials;
- Families being accused of fabricating their daughters’ illnesses;
- Inadequate duty of care from health care officials;
- Lack of knowledge by medical doctors and consultants on how to recognize and treat the vaccine injured;
- Medical doctors who believe illnesses were caused by the HPV vaccines but are too afraid to speak out.
This sadly is how it is in the UK at the present time. A very important point was made below, ‘these are real people in real situations and it does not matter whether it is a Conservative or Labour government, as politicians you are elected to speak on our behalf and work on our behalf at all times.’

All these families ask for is to be respected, to be listened to and, most importantly, to be believed.
The undernoted presentations were given by girls who were injured by an HPV vaccine and parents speaking on behalf of their daughters.
Julie Jones, mother of Stacey Jones, Bilston, Midlands:
My daughter Stacey had her first Cervarix vaccine on 15th November 2008, aged 17, and we noticed that her mood changed following this vaccination. After the second jab in January her aggressive behaviour was more noticeable and then after her third vaccination in May 2009 she became very disorientated which increased in intensity, couldn’t sleep and that was followed by partial seizures which then developed into full blown seizures.
There were many serious faults here with the NHS, not treating our daughter correctly, sending her to a psychiatric hospital which could not help her but thankfully they recognised her illness was a medical illness and she was sent home.
New Cross Hospital at that time let us down badly and that was when I made contact with my MP, Pat McFadden. Pat gave my family a lot of support for which we are very grateful. Over a period of time Stacey was allocated a place at the Brain Injury Rehabilitation Trust – Stacey spent 12 weeks there relearning simple tasks and she was also assigned a neurologist from the Queen Elizabeth Hospital in Birmingham.
Stacey was officially diagnosed with Anti-NMDA receptor encephalitis – an autoimmune form of encephalitis – NOT VIRAL ENCEPHALITIS. According to NHS Choices, in ‘rare’ cases this condition has followed vaccination. It is strange then that at the same time a young girl called Paige Brennan also from the Midlands was vaccinated with Cervarix and was also diagnosed with the same autoimmune condition as Stacey – not so rare after all.
Now after five years of great improvement in Stacey’s health and being able to go to University, we are devastated that she has had a re-occurrence of this autoimmune form of encephalitis – Stacey was admitted to hospital where she received the best of treatment which was so much better than the last time – I can report she has just been allowed to go home with further rehabilitation to take place. What does the future hold for our daughter – according to the MHRA there are no serious adverse reactions to the Cervarix vaccine – well that is not the case.
Ashleigh Cave, Liverpool:
My name is Ashleigh Cave and I received the HPV Cervarix injection in October 2008 when I was twelve years old. Within an hour of having the injection I had extremely bad headaches. I was going for a routine doctor’s appointment and the doctor said I was suffering from possible side effects of the vaccine and that I should start to feel better in the next forty eight hours. Only I never and over the course of the next week I suffered from severe flu like symptoms and I had no energy to stay awake.
My legs became so weak that I was admitted to hospital as I couldn’t walk or move my legs. I suffered with excruciating pain and was put on a concoction of eight different painkillers. I had tests, scans and x-rays yet they all came back inconclusive. At this point, the doctors didn’t know what was wrong and came to the conclusion that my health issues were psychosomatic. I had to have a full psychiatric assessment which came back in my favour that my health problems were not in my head. So their next move then was to try and blame my mum. They got social services involved and we were threatened that I would be taken into care if my mum did not stop speaking to the press. All in all I was in Alder Hey Children’s hospital for twelve months where I had intensive Physio and Hydrotherapy sessions daily.
I can now walk, however I am limited as I have never fully regained the strength back in my legs. I had health problems before I had the injection, such as Noonan syndrome, pulmonary stenosis, bronchomalacia, bladder problems and chronic asthma. Since I had the injection, everything I previously suffered with was intensified. I have had three surgical procedures to try and help my bladder so I do not have to rely on self-catheterising and administering treatment weekly and I am constantly picking up every cold that is going meaning I am quite frequently in hospital as it affects my chest.
Every girl who has had a reaction has had different health backgrounds, some having previous medical problems and some having a clean bill of health. Some girls have been affected in different ways ranging from paralysis, to having seizures daily but the one thing we all have in common is the fact we have all received this injection. The past five and a half years have been horrendous for me and my mum but what makes it worse is the fact that girls are still having this injection and are still being damaged.
How many more girls have to go through this before someone will take notice and listen? How many more families have to be blamed before being offered support and finally how many more lives have to be turned upside down before we get the recognition and medical help we need for what we are going through?
Emily Ryalls, Ossett, W. Yorkshire:
Hello, my name is Emily. I’m 16 years old and have just completed my GCSE year in high school.
I’d like to thank you for this opportunity to share my experience of the HPV vaccination as well as being able to speak on behalf of other girls. I’m incredibly nervous, as you can probably tell, but so grateful for you taking the time to listen to me today.
I had the HPV vaccination 3½ years ago. I became ill after the first jab, the 2nd jab worsened my condition and after the third jab the visits to A&E started. At first I had complete faith in doctors. Then I was labelled with ME/CFS and I realised this meant that doctors didn’t know what to do with me.
I was so ill, I was missing lots of school, missing my friends and the only treatment given was to see a psychologist. My paediatrician wanted me under the care of a psychiatrist. Every doctor I saw refused to consider vaccine damage and none of them reported it.
After 2 years and a lot of research, we found a specialist who confirmed I had POTS – Postural Orthostatic Tachycardia Syndrome, which is a dysfunction of the autonomic nervous system. Everything that the body should do automatically doesn’t work properly for me, especially when I’m sitting or standing up. It affects every part of my body – eyesight, heart rate, breathing, blood pressure, digestion and especially cognitive problems, which I hate the most because I often feel humiliated in school and it’s affected my education so much.
I’m finally under a neurologist who is trying to help me and who has confirmed my POTS is a result of vaccination.
The only thing that has got me through the last 3 years has been the support of my mum and family and having such a great group of friends. I can’t begin to imagine how hard it is for the girls who don’t have this support.
Although as a group, we all have different stories; we all share the HPV vaccination as the trigger. The question is how many more girls have to go through this before something is done?
Thank you.
Brianna Price, Newport Pagnell:
I’m Brianna, and I’m 15 years old. I had my first and only dose of Cervarix in September 2011, when I was 12 years old. I then experienced my first symptoms 3 weeks after in October, when I’d just turned 13. I went to my GP and had a wide range of tests done but they all came back negative. 6 months later I was diagnosed with CFS/ME by a Great Ormond Street consultant.
Before the jab I’d represented my school in athletics and won them medals, been dancing since I was 2 – I’ve now had to stop this, performed at the Royal Albert Hall and even done some TV work in a BBC drama series.
In the beginning of being ill I was bullied at school. I had people laughing at me, saying I was faking, and even hurtful comments like ‘why aren’t you dead yet?’ I’ve lost all of my friends but one friend because I wasn’t in school and I couldn’t go out with them so now I’m just not invited anymore. It has taken 2 ½ years to get me from 0% attendance to 30% in school, with me doing 12 hours a week maximum.
I have 6 monthly paediatrics and Great Ormond Street check-ups and monthly psychology and physiotherapy sessions. (I got discharged from CAMHS because it wasn’t helping). I have to take tablets to sleep. If I don’t take the tablets I don’t sleep at all that night. I also have chronic back pain which I’m on medication for and when it’s at its worst I can’t breathe properly because of it.
Since then I have also been diagnosed with Raynaud’s, hypermobility and postural hypertension.
My mum thought it was the best idea to allow me to get the vaccine, but if we knew then what we know now about it, I would never have had it.
When we first saw the Great Ormond Street consultant we asked him did he think the vaccine had caused my illness. He replied, “All I can say is I’m treating a lot more girls following the vaccine.”
Presentation with reference to the autoimmune condition Alopecia:
(For the sake of her daughter, mum is not sharing her name – but she presented in full to the Shadow Minister)
My daughter is 13- the youngest of our 3 children. She has 2 older brothers aged 18 and 21. We are a very close knit, fun loving, happy family and all 3 children are extremely close.
Sport and particularly swimming is in the family, the lads have won medals at national level and my daughter has club records. She also has a gold medal for gymnastics and trampolining. She used to play water polo for fun.
She had her 3 Gardasil HPV immunisations, for genital warts, in October 2012 then January and April 2013. On each occasion she had a significant reaction and with hindsight we wouldn’t have let her have number 2 and 3 but we can’t turn back the clock now! She was lethargic, had muscle fatigue, lost her appetite, stopped her beloved sport and had time off school (unheard of) and her periods stopped. In April 2013 following her 3rd jab her hair started falling out in clumps, she lost her eyebrows, lashes and by the summer of 2013 she was totally bald.
I want to share with you the medical professions reaction as I believe this helps mask the bigger HPV picture…
One Dr said and I quote, “These things happen and Jemma needs to move on…”
Another, “This is quite common around the 12/13 year age group”…not surprising in my mind since this is when the immunisation is given.
When confronted with the possible link, the doctor was extremely dismissive and didn’t offer the opportunity of yellow carding the vaccination (which I believed was meant to be a procedure carried out post thalidomide). I did this under my own steam and told him retrospectively what I had done. I was not popular for taking this course of action.
This may be why the recorded numbers of side effects are quite low…..you have to be proactive….
Friends who are GPs have said off the record that Gardasil was and is the cause of her ill health; but for fear of the backlash are not prepared to put their heads above the parapet.
In summary, she no longer does any sport, her school attendance is poor due to total lack of energy, and she sleeps 14+ hours a day and her periods have still not started. Her lack of hair has turned her from a fun loving outgoing and positive person into a self-conscious and reclusive child.
We have explored every avenue for antidotes and suggested courses of action but this has been done with no backing from the very people who should be there to support us.
Clare Ramagge, Reigate, Surrey:
In 2009, Dr Jawad paediatric consultant, demanded why I had allowed my daughter to have the third Cervarix vaccination? We were advised that he had previously highlighted the link between the vaccination and side effects of arthralgia and he verified this concern to Crispin Blunt MP for Reigate. Mr Blunt successfully secured a debate in Parliament to highlight the fact that formally fit healthy young girls were experiencing a number of severe adverse reactions. He highlighted the fact that there was a lack of a robust compensation scheme or mandatory warning system to report such adverse reactions and he questioned the suitability of school as an environment in which to vaccinate children.
In Rebecca’s case, when standard treatment did not cure her, concerned paediatricians brought in multi-disciplinary teams. As described by Dr Leonard Jason, social psychologist,”As a group otherwise caring professionals can commit acts of cruelty that they would not be capable of as individuals.”
We were threatened with legal action if we did not agree to her being sent to a lock up psychiatric unit for eating disorders even though she did not have an eating disorder. They tried to put different labels on her but never diagnosed a psychiatric problem and tried to Section her. After 16 months, a new social worker to Rebecca’s case, with the advice of Dr Nigel Speight, Lady Mar and a solicitor secured Rebecca’s discharge from the unit. Rebecca is still very poorly but being cared for at home by her family, GP, Nurses, nutritionist and a consultant lead. This consultant, an immunologist who also specialises in ME/CFS, explained to the GP that it is likely that it was the Aluminium in the vaccine that triggered Rebecca’s very severe ME.
On all of Rebecca’s notes there is reference to her deterioration starting straight after the first vaccination. 2 consultants have made reference to the vaccine, one to query why she had been allowed to follow through with it and the other to point out the link with Aluminium being the trigger. Rebecca will never get back the 6 years she has lost as a consequence of having this vaccine and we as a family will never recover from the treatment we have received from some of the so called professionals involved in this case. Rebecca remains positive and hopeful of a recovery but like all the other girls affected, she deserves to have recognition as to the vaccine being the cause, she deserves better treatment and better support.
Points raised by Steve Hinks, Carol Green and John Ramagge:
Steve Hinks:
Before the meeting with Luciana Berger, MP, Shadow Minister for Health we held a pre-meeting with other political representatives. During the discussions we were advised that our daughters are what are known widely as ‘vaccine collateral damage’ i.e. unintended casualties. We were grateful for this open and honest comment which is certainly not typical of the Department of Health and National Health Service because most of the families have been told many times, and in writing, that this vaccine is safe and the many side-effects reported are not attributable to the vaccine. In fact many families are blamed for causing the unexpected and inexplicable illnesses and investigated for Fabricated or Induced Illness (FII, previously known as Munchausen’s Syndrome by Proxy). Not content with turning the blame on parents many NHS health professionals have told blatant lies to FII investigators which can be proven by their own material evidence obtained under the Freedom of Information Act (FOIA).
We were also advised to sum up our expectations in a maximum of just two points for maximum effect, rather than a long list.
- Point 1: The DoH and NHS must share the truth and facts related to the HPV vaccine and investigate the unexplained illnesses rather than blame the parents. These investigations should be coordinated at national level. We have many examples of statements in writing from Health Directors and Consultants that this vaccine is safe and not the cause of the adverse reactions, yet the number of Yellow Card reports to the Medicines and Healthcare Products Regulatory Agency (MHRA) is 10 – 100 times more than for the other common vaccines. Statistics obtained from the MHRA under the FOIA were presented to Ms Berger. In 5 years the number of reported reactions to HPV vaccine is 16,726 of which 2,661 are considered serious, including four deaths. Parents also highlighted that they had been discouraged from raising Yellow Cards.
- Point 2: Collateral damage arises in different quantities – it can be small or large and those agencies involved in collateral damage usually at least take preventive action to reduce and minimise it. Given the data reported to the MHRA it is evident that the quantity of reactions reported by Yellow Card are significantly more than for any other vaccine and therefore the use of this vaccine must be stopped until it can be proven to be ‘reasonably’ safe. It must be remembered that this vaccine is expected to reduce incidence of cervical cancer but so far there is no evidence that it will and, since it is accepted that it is not effective against over 15 types of HPV which can cause cervical cancer, the Smear Test will always have to be in place, irrespective of immunisation. This test is safe, extremely efficient and cost effective.
Carol Green, mother of injured young woman Katie:
For the Minister to consider that a consultation by the NHS and government should be a top priority in order to review guidelines when a child presents at hospital or GP surgery with a possible adverse reaction to a vaccination. If this was to become a reality, rather than being dismissive, there would be a set of clear procedures for physicians and doctors to follow to establish whether the vaccine was the likely cause or not. Then appropriate treatment and support (both emotional and financial) can be given to the children and their families so that they would not have to endure what so many families have gone through since the HPV vaccination programme was introduced in the UK in 2008.
As the HPV programme had been promoted and underwritten by the government, they are responsible for ensuring these children receive adequate recognition and compensation if the vaccine is considered to be the cause of their injuries.
John Ramagge:
John pointed out to the Minister that his MP, Crispin Blunt had introduced his daughter’s case to parliament in May 2009 and at that time Labour was in government. This had followed the Minister’s claim that as she was not in government at the present time, there was little that she could do. In 2009, the very questions and points raised by Crispin were belittled by Dawn Primarolo but John wished to make the Minister realise that although she is in shadow government at the moment, as a politician she and her colleagues need to take this matter seriously. These are real people in real situations and it does not matter whether it is a Conservative or Labour government, as politicians you are elected to speak on our behalf and work on our behalf at all times.
All that families ask is to be respected, to be listened to and, most importantly, to be believed.
As one politician recently said, ‘There are only so many times you can say that this is a coincidence’. He is right.
We do hope now that similar meetings for families with injured girls can be arranged with Jane Ellison, Minister for Public Health. This would give the families the opportunity to share their experiences also with the Government Health Team. The Shadow Health Team treated our families with great courtesy and with compassion and it would be excellent if both Health Teams could discuss this issue amongst themselves as this is a national issue and one to be taken seriously.
Gut bacteria linked to autism#ASD#iBelieve#Vaccines
By Dr Flannery 
The digestive tract is home to more than 100 trillion microorganisms. That’s ten times the number of cells in the human body! Although humans can survive without these tiny guests, they perform a host of useful functions, such as fermenting unused food, preventing growth of harmful bacteria, producing vitamins, and training the immune system. But did you know the bacteria in your gut can affect your brain, too? In fact, recent research on the gut has found some interesting links between the gut microbiome – the complex and unique microbiological community within the gut –- and autistic behavior in children.
As parents well know, children with autism have a high rate of problems with gastrointestinal (GI) disorders. The resulting discomfort can worsen behaviors and interfere with their ability to participate in, and benefit from, activities of daily life, education, and therapeutic activities.
On a related note, it has been known for some time that children with autism tend to have abnormal and less diverse communities of gut bacteria than children without autism. Recent research on children with autism has revealed these interesting facts:
Their intestinal cells show abnormalities in how they break down and transport carbohydrates, which can affect the amount and type of nutrients these cells provide to intestinal bacteria. This in turn may alter the makeup of the intestine’s normal community of digestive bacteria — with ill result.
Their intestines are home to abnormal amounts of certain digestive bacteria that contribute to digestive problems, intestinal inflammation, and more severe autism symptoms.
There are lower levels of three important gut bacteria; Prevotella, Coprococcus, and Veillonellaceae.
Theory has it that the community of bacteria in the gut affects the immune system, which then sends messages to the brain. This may explain why parents of children with autism report that special diets and probiotics (nutritional supplements containing “good” bacteria) improve their children’s digestion as well as their behavior.
The Gut-to-Brain Connection
The most recent research on the connection between the gut and autism explores how the gut microbiome affects the autistic brain. Researchers at Arizona State University found that concentrations of metabolites (byproducts) from seven specific bacteria are more prevalent in autistic children’s fecal samples. According to study author Dae-Wook Kang, “Most of the seven metabolites could play a role in the brain … We suspect that gut microbes may … affect gut-to-brain communication and/or alter brain function.”
Of the seven metabolites that were noticed, three warrant special note for their apparent relation to brain function, thereby behavior:
Homovanillate was present at lower levels in children with autism; it is normally produced when dopamine (an important brain neurotransmitter involved in many aspects of mood and behavior) is broken down.
N,N-dimethylglycine was found at lower levels; it has been used before to decrease autism symptoms.
The ratio of glutamine to glutamate was higher: these are metabolized into GABA, a vital inhibitory neurotransmitter associated with relaxation. An imbalance between glutamate and GABA transmission has been associated with autistic-spectrum type behaviors such as hyper-excitation.
These connections offer insight into possible link between the gut biome and the behaviors seen in autistic children. Researchers say they would like to conduct a clinical study using fecal transplants from healthy donors to see if normalizing an individual’s community of gut bacteria would reduce autism symptoms.
Although the study was small, it adds to the growing body of research that tells us the gut is closely tied to the brain.
France: Meeting to debate HPV vaccines, Gardasil and Cervarix#vaccines#IBelieve#HPV

Paris, 23 June 2013: A three hour discussion was held during which various medical professionals, politicians, and health authorities had the opportunity to openly debate serious concerns about the HPV vaccines Gardasil and Cervarix.
Dr. Philippe de Chazournes recently sponsored an open letter to the French Minister of Health calling for the establishment of a parliamentary mission to investigate various aspects of HPV vaccination campaigns. (more information here) Over 200 medical professionals signed the letter confirming their agreement with the stated concerns about the safety, efficacy, and necessity of using Gardasil and Cervarix in national cervical cancer prevention programs.
Michele Rivasi, MEP, chaired roundtable discussions pertaining to the questions raised in Dr. de Chazournes’ letter to the French Health Ministry.
Stakeholders representing both sides of the debate were invited to attend as well as members of the French Parliament, representatives from Sanofi-Pasteur MSD, and national health authorities. Drs. G. Delepine, N. Delepine, A. Siary, Cl-Michal Teitelbaum, JP Hamon, and Mr. Coletti were in attendance along with many other interested parties.
The topics open for discussion are as follows:
- What is the justification for HPV vaccination programs?
- What is the risk/benefit profile of Gardasil and Cervarix?
- What place do HPV vaccines have in cervical cancer prevention strategies, and at what cost?
- Gardasil: Cervical Cancer or Political Cancer?
- What is the level of ’ethical care’ in the new ’cancer plan’?
Member of the European Parliament, Michéle Rivasi, opened the meeting with the following speech, eloquently stating the actions necessary to protect the public health as well as public health funding.
To paraphrase her words, these vaccines are unnecessary, dangerous to many, and certainly a huge drain on precious public health funds. To halt HPV vaccination programs, pending intense investigation and proof of stated purpose could very well be the salvation of our young people.
Presentation by Michele Rivasi, European Ecology MEP
Translation by Helen Kimball Brook
It is an honor for me to receive Dr. Philippe de Chazournes today in the Parisian offices of the European Parliament. Dr. de Chazournes has fought long and hard as spokesperson for doctors in the current scandal linked to the Gardasil vaccine, the famous Sanofi-Pasteur MSD vaccine against certain strains of the human papillomavirus which can cause cancer. A large number of doctors have signed his open letter to Marisol Touraine, French Minister of Social Affairs, expressing their fears around the idea of doubling the vaccination rate of young girls with a vaccine whose effectiveness is scientifically controversial. Some of them are here today and I thank them for being here. They are demanding a parliamentary mission to clarify this question. Last April, I personally made a public demand for a moratorium, i.e. an end to mass vaccination with this vaccine until in-depth research can be performed on its benefits, risks and effectiveness.
Vaccine safety, as a general rule, is being increasingly questioned. Between 2005 and 2010, the proportion of French people in favour or very in favour of vaccination dropped from 90% to 60% (2013 INPES Peretti-Watel health barometer). The percentage of French people between the ages of 18 and 75 who are anti-vaccination increased from 8.5% in 2005 to 38.2% in 2010. In 2005, 58% of doctors questioned the usefulness of vaccines administered to children while 31% of doctors were expressing doubts about vaccine safety. These figures must surely have increased since then.
Alongside this dramatic slump in confidence, research carried out worldwide – here in France by R. – K. Gherardi and F.-J. Authier, in Canada by C. Shaw and L. Tomljenovic, in North America by S. Seneff and S.-H. Lee, in Israel by Y. Shoenfeld and in the UK by C. Exley and others – blames the toxicity of the aluminium salts used as adjuvants in vaccines.
The injection of these aluminium salts could be the cause of the considerable and unexplained increase in the number of pathologies reported because they migrate through the body until they reach and accumulate in the brain. In certain predisposed individuals, very serious adverse effects have been observed following vaccination: death, convulsions, fainting, autistic disorders, Guillain-Barre syndrome, transverse myelitis, facial paralysis, chronic fatigue syndrome, autoimmune diseases, pulmonary embolisms, macrophagic myofasciitis, pancreatitis and others.
It was the work of E3M, an organisation formed by macrophagic Myofasciitis victims, which encouraged me to bring this subject up within the European Parliament. Macrophagic myofasciitis is a little known but extremely disabling disease caused by the aluminium salts in vaccines.
Without being totally against the actual principle of vaccination, I feel that it is absolutely essential for specification of our vaccine policy to reflect the greatest of transparency and that the voices of vaccine victims be heard so that appropriate responses may be given and solutions found: in particular, urgent and abundant research financing and provision of a basic vaccine which is aluminium-free.
I therefore invited scientists and specialists in this area to come speak to us about their work on Gardasil during a press conference held at the Parisian offices of the European Parliament, last April.
Over the last seven years, nearly two million young women between the ages of 13 and 26 have received at least one dose of this vaccine, 65% of which is reimbursed by the French Social Security… but its effectiveness has still not been proven. Since then, an increasing number of young girls have been claiming that it has made them ill and the matter is becoming an issue Europe-wide.
Marisol Touraine, French Health Minister, has nonetheless just re-affirmed her attachment to this vaccination by confirming the 2014 recommendations which advise “all young girls between the ages of 11 and 14” to get the HPV vaccine. The message was apparently not heard.
Worse still, in early May, EMA (European Medicines Agency) experts recommended that the Gardasil HPV vaccine indication be lowered to age 9 for prevention of anal cancer and pre-cancerous anal lesions. One of the arguments used for this was that there are 6,800 new anal cancers in Europe every year. This feels to me like an attempt to find new justifications for the overall recommendation of Gardasil.
The French government needs to save 50 billion Euros over the next three years and ten of those billions must be saved in Health Insurance. Widespread administration of Gardasil would cost 926 million Euros (i.e. 9.3% of the needed health insurance savings) over three to four years, this for the catch-up campaign alone.
To stop this plan would be a genuine move for public health: this vaccination is worthless, clearly dangerous and a financial black hole. It serves no purpose for the European Medicines Agency to rush to the aid of Gardasil by recommending its use in the prevention of anal cancer (which causes fewer than 200 deaths every year in France, which is 0.11% of all cancer deaths).
What does Europe want? How is it that we ask the member States to reduce their deficits while simultaneously inciting them to spend more and more for the greater good of the pharmaceutical industry? How is it possible that we ask the French (and Europeans because the situation is exactly the same in many countries) to “tighten their belts” while asking them to hand over such large gifts to Big Pharma at the same time?
We must ask ourselves these questions and continue to fight against the health scandals of today and tomorrow by demanding absolute transparency in these highly sensitive issues.
Learn more about the issues here.
View the entire press package in French here.
The SaneVax Team would like to thank all of the participants in this debate. We sincerely hope every country in the world holds similar events. If HPV vaccines are as safe and effective as advertised, public scrutiny should be no problem.
Until such time as open and honest scientific debates are allowed in every country, medical consumers need to remember – RESEARCH BEFORE CONSENT – you can’t unvaccinate.
Frank B. Engley, Jr., PhD – A Pioneer in the research of Thimerosal Efficacy and Toxicity#Vaccines#ASD#IBelieve
“Apparently the medical profession does not read the safety data sheets provided by Lilly and other chemical manufacturers made available to physicians, pharmacies, hospitals and health departments. It states for thimerosal: toxic, mutagen, allergen, hypersensitivity, alters genetic materials, may cause mild to severe mental retardation, may cause mild to severe motor coordination, all sounds a lot like autism.”
Frank B. Engley, Jr., PhD, by Eric Gladen and David Ayoub, MD